
Diploma Course in Aesthetic Dermatology & Skincare
Course Duration : 2 Days
Course Target : Diploma Course in Aesthetic Dermatology & Skincare
Faculty : Dr. Refazul Alam (refat) , Dr. Jinat Khan, Dr. Nizhum Ahmed, Dr. Syeda Maria Adnin , Dr. Afnan H Tanna,
Open to All MBBS Students undergoing Internship , MBBS & BDS.
CPD certificate in Diploma Aesthetic Dermatology & Skincare will be awarded.
| DAY 1: 03rd July 2025 (Thursday) Skin Development Anatomy & Physiology, Clinical Dermatology & Laser Machine Orientation | |
| 09:15 – 09:30 | Collection of Lecture Course Notes |
| 09:30 – 11:30 | Introduction to Glutathione, Routes of Administration & Dosage Guidelines, Introduction to conclusion on Hair Transplantation with Hands-on Training |
| 11:30 – 11:45 | Morning Tea Break |
| 11:45 – 01:30 | Introduction to Conclusion on Face & Acne Scar Formation & Types, Advanced Treatment for Hypertrophic & Keloid Scars, Patient Selection & Consultation |
| 01:30 – 02.00 | Multiple Choice Question Quiz on Glutathione & Face Scar formation. |
| 02:00 – 02:30 | Lunch Break |
| 03:00 – 17:30 | Hands on training & Live Demostration on Face & Acne scar |
| DAY 2: 4th July 2025 (Friday) PRP (Platilet Rich Plasma), Microneedling | |
| 09:15 – 09:30 | Collection of Lecture Course Notes |
| 09:30 – 11:30 | Introduction to conclusion of Botulinum Toxin, Details (Anatomy & Physiology, Indications & Applications, Injection Techniques & Dosage, Introduction to conclusion of Dermal Filler, Details (Introduction to Dermal Fillers , Facial Anatomy & Injection Safety, Indications & Applications, Injection Techniques & Product Selection, Managing Complications & Side Effects) |
| 11:30 – 11:45 | Morning Tea Break |
| 11:45 – 01:30 | Introduction to conclusion of Filler & Thread, Details of Advanced Filler & Thread Types & Their Uses, Advance Facial Anatomy & Injection Safety Indications & Applications, Patient Selection & Consultation, Filler & Thread Placement Techniques, Managing Complications & Side Effects & Emergency Protocol. Introduction to conclusion of Laser Technology, Types of Lasers Used in Aesthetic Dermatology |
| 01:30 – 02.00 | Multiple Choice Question Quiz on Botox, Filler, Thread & Laser. |
| 02:00 – 02:30 | Lunch Break |
| 03:00 – 17:30 | Live Demonstrations and Hands-On Training Workshops. Certificate Handover |
Diploma Course in Aesthetic Dermatology & Skincare
Day 01
- Glutathione
- Hair Transplantation
- Face & Acne Scar
- Introduction of Glutathione
Glutathione (GSH) is a tripeptide composed of:
- Glutamic acid
- Cysteine
- Glycine
It is one of the most abundant intracellular non-enzymatic antioxidants, present in nearly all living cells, and plays critical roles in detoxification, redox balance, immune function, and cellular protection.
2. Structure of Glutathione
- Molecular Formula: C₁₀H₁₇N₃O₆S
- Structure: γ-L-glutamyl-L-cysteinylglycine
- Unique Bond: Gamma peptide linkage between glutamate and cysteine (unusual γ-peptide bond instead of the usual α-peptide bond)
3. Biosynthesis of Glutathione
Occurs intracellularly in two ATP-dependent steps:
Step 1:
γ-glutamylcysteine synthetase
- Combines glutamate + cysteine
- Rate-limiting step
- Regulated by feedback inhibition by GSH
Step 2:
Glutathione synthetase
- Adds glycine to form glutathione
Location: Predominantly in the liver, also in kidneys, lungs, and intestines.
4. Forms of Glutathione
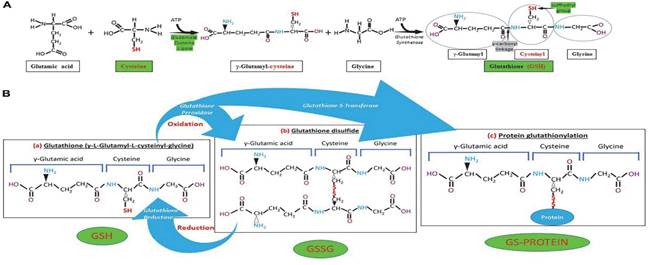
| Form | Description |
| GSH | Reduced glutathione (active antioxidant form) |
| GSSG | Oxidized glutathione (2 GSH molecules joined via disulfide bond) |
- Healthy GSH:GSSG ratio = >100:1 in cytosol
- Decrease in this ratio = oxidative stress marker
ii. Medical & Aesthetic Uses of Glutathione
1. Liver Disorders
- Mechanism: Detoxifies hepatotoxic substances; replenishes hepatic GSH stores.
- Indications: Alcoholic hepatitis, NAFLD, drug-induced hepatitis (e.g., paracetamol toxicity), viral hepatitis (supportive).
- Form: Oral or IV
2. Neurodegenerative Diseases
- Mechanism: Protects dopaminergic neurons from oxidative damage.
- Indications: Parkinson’s Disease, Alzheimer’s Disease (supportive therapy).
- Evidence: Studies suggest slowed disease progression in Parkinson’s.
3. Chronic Kidney Disease (CKD)
- Mechanism: Reduces oxidative stress and inflammation in renal tissues.
- Adjunct: Used along with other nephroprotective agents.
4. Diabetes Mellitus
- Mechanism: Reduces insulin resistance via antioxidant effect.
- Application: Supports glucose metabolism and protects pancreatic β-cells.
5. Autoimmune & Inflammatory Disorders
- Mechanism: Modulates immune activity through cytokine and T-cell regulation.
- Applications: Lupus, rheumatoid arthritis (experimental/supportive).
6. Pulmonary Diseases
- Indications: ARDS, cystic fibrosis, and COVID-19 (investigational use).
- Route: Nebulized GSH is being studied for direct pulmonary antioxidant effects.
7. Cancer (Supportive Use)
- Use: Protects normal tissues from chemotherapy-induced toxicity.
- Caution: May protect tumor cells—must be used judiciously and under oncologist supervision.
Aesthetic (Cosmetic) Uses of Glutathione
1. Skin Lightening / Brightening
- Mechanism:
- Inhibits tyrosinase (enzyme for melanin synthesis)
- Promotes pheomelanin (light pigment) over eumelanin (dark pigment)
- Antioxidant effect reduces UV-induced melanogenesis
- Effect: Gradual skin lightening, more noticeable in Fitzpatrick I–IV
- Form: Oral, IV, liposomal, topical (limited absorption)
2. Melasma & Hyperpigmentation
- Mechanism: Reduces oxidative stress that exacerbates pigmentation
- Effectiveness: Best with combination treatments (e.g., tranexamic acid, laser)
3. Anti-Aging
- Mechanism: Slows cellular aging by reducing free radical accumulation
- Result: Improved skin elasticity, reduced fine lines (limited clinical data)
4. Acne & Post-Inflammatory Hyperpigmentation (PIH)
- Mechanism: Anti-inflammatory and antioxidant effects reduce lesion severity and pigmentation
- Benefit: Improved healing and reduced post-acne marks
Limitations & Ethical Considerations
| Concern | Notes |
| Regulatory Approval | IV glutathione for skin lightening is not FDA-approved |
| Overuse Risks | Long-term high-dose IV use may suppress natural GSH synthesis |
| Unrealistic Expectations | Skin lightening takes months and varies by skin type |
| G6PD Deficiency | Risk of hemolysis—screen before IV use |
| Lack of Standard Protocols | Dosing and duration not standardized in aesthetic practice |
Functions of Glutathione
A. Antioxidant Defense
- Neutralizes reactive oxygen species (ROS) and free radicals
- Regenerates Vitamin C and Vitamin E
B. Detoxification
- Conjugates with toxins and xenobiotics (via glutathione-S-transferase) for renal excretion
C. Redox Signaling
- Maintains intracellular redox homeostasis
- Regulates transcription factors (e.g., NF-κB, AP-1)
D. Immune Modulation
- Enhances T-cell proliferation, antigen presentation, and NK cell activity
E. Protein and Enzyme Regulation
- Reduces disulfide bonds in proteins (maintaining proper folding)
F. Skin Pigmentation
- Inhibits tyrosinase enzyme (blocks melanogenesis)
- Converts melanin production from eumelanin (dark) to pheomelanin (light)
Routes of Administration
| Route | Pros | Cons |
| Oral | Convenient, available as tablets | Poor bioavailability due to GI breakdown |
| IV | Fast action, 100% bioavailability | Risk of allergy, controversial long-term use |
| Sublingual | Better absorption than oral | Limited data |
| Liposomal | Enhanced oral bioavailability | More expensive |
| Nebulized | Used in respiratory support | Limited clinical approval |
IV. Indications
Glutathione therapy may be administered in the following medical and aesthetic contexts:
A. Medical Indications
| Condition | Rationale |
| Liver diseases (e.g., alcoholic hepatitis, NAFLD, drug-induced hepatitis) | Protects hepatocytes from oxidative damage, supports detoxification |
| Chronic kidney disease (CKD) | Reduces oxidative burden in renal tissues |
| Parkinson’s Disease | Preserves dopaminergic neurons from oxidative degeneration |
| Diabetes Mellitus | Helps lower oxidative stress, supports insulin sensitivity |
| Autoimmune disorders | Modulates immune responses via redox control |
| COVID-19 / ARDS (experimental) | Reduces oxidative inflammation in lung tissues |
| Cancer (supportive care) | Protects normal cells during chemotherapy (controversial role in tumors) |
B. Aesthetic Indications
| Concern | Use |
| Skin brightening/lightening | Inhibits melanin synthesis and tyrosinase activity |
| Melasma, hyperpigmentation | Reduces oxidative stimulation of melanocytes |
| Anti-aging | Slows oxidative cellular damage contributing to aging |
| Detox/Wellness protocols | Popular in wellness and IV drip clinics for “cellular cleansing” |
General Safety Profile
Glutathione is endogenously produced in the human body and is generally well tolerated when used in physiological or therapeutic doses. However, adverse effects may arise due to inappropriate dosing, incorrect administration routes, or individual susceptibility (e.g., genetic conditions like G6PD deficiency).
- Common Side Effects
| Route | Side Effects | Frequency |
| Oral | Abdominal cramps, bloating, metallic taste | Uncommon |
| IV | Headache, dizziness, flushing, nausea, mild rash | Occasional |
| Inhaled | Cough, chest tightness, bronchospasm (especially in asthmatics) | Rare |
| Topical | Contact dermatitis, allergic rash | Rare |
2. Serious Adverse Effects
Although rare, the following complications can occur, particularly with high-dose IV glutathione:
A. Anaphylaxis
- Symptoms: Rash, difficulty breathing, hypotension
- Onset: Minutes after IV administration
- Risk Factors: History of drug allergies, IV bolus injections
B. Bronchospasm
- Most common in patients with asthma or COPD
- May occur with inhaled or IV forms
C. Renal Stress
- High doses may cause osmotic stress on the kidneys
- Monitor renal function in patients with pre-existing CKD
D. Hemolysis in G6PD Deficiency
- Mechanism: Glutathione recycling impaired, leading to red cell damage
- Screening: G6PD testing mandatory before IV therapy
3. Controversial & Unproven Risks
| Risk | Evidence Level | Comment |
| Skin cancer risk | Theoretical | No clinical proof, but altering melanin balance is debated |
| Tumor progression support | Experimental | GSH protects all cells—may reduce chemotherapy efficacy |
| Infertility | Minimal | Anecdotal only; no solid clinical correlation |
4. Overdose & Toxicity
While no established lethal dose exists for glutathione, excessive or prolonged use can lead to:
- Disruption of redox balance
- Rebound oxidative stress upon withdrawal
- Unknown long-term aesthetic effects
5. Contraindications
| Condition | Reason |
| G6PD deficiency | Risk of hemolytic anemia |
| Severe asthma | Risk of bronchospasm |
| Allergy to glutathione/sulfur | Potential for hypersensitivity |
| Pregnancy & lactation | Insufficient safety data |
6. Safety Recommendations for Clinical Use
- Screen patients for G6PD deficiency
- Perform a patch test for topical application
- Use slow infusion for IV administration (avoid bolus)
- Avoid unregulated high-dose IV regimens
- Always obtain informed consent, especially for aesthetic use
- Educate patients about realistic expectations and possible adverse effects
7. Regulatory Status & Ethical Considerations
| Aspect | Notes |
| FDA approval | Approved for liver disease and acetaminophen toxicity |
| IV skin lightening use | Not FDA-approved; off-label and controversial |
| Marketing caution | Many cosmetic clinics make unproven health claims |
| Ethical use | Medical justification must outweigh cosmetic demand |
Clinical (Medical) Combinations
A. With N-Acetylcysteine (NAC)
- Use: Hepatic protection, detox, oxidative stress
- Rationale: NAC is a glutathione precursor that replenishes intracellular stores
- Example: Acetaminophen overdose, alcoholic hepatitis
B. With Alpha-Lipoic Acid (ALA)
- Use: Diabetes, neuroprotection, detox
- Rationale: Both are antioxidants; ALA recycles GSH and reduces oxidative inflammation
C. With Vitamin C & E
- Use: Chronic diseases, immune modulation
- Rationale: Synergistic antioxidant effect; Vitamin C helps regenerate glutathione from oxidized form (GSSG)
D. With Chemotherapeutic Agents (Cisplatin, Doxorubicin – Supportive)
- Use: Cancer (supportive care)
- Rationale: Protects healthy cells from chemotherapy-induced oxidative damage
- Caution: May protect tumor cells—only under oncologist supervision
Aesthetic (Cosmetic) Combinations
A. Glutathione + Vitamin C (Ascorbic Acid)
- Use: Skin lightening, melasma, anti-aging
- Rationale:
- Vitamin C stabilizes glutathione in plasma
- Enhances tyrosinase inhibition
- Route: IV, oral, or topical
B. Glutathione + Tranexamic Acid
- Use: Melasma, PIH (post-inflammatory hyperpigmentation)
- Rationale: TXA inhibits melanocyte-stimulating pathways; works well with GSH
- Route: Oral or mesotherapy
C. Glutathione + Glutamine + Collagen Peptides
- Use: Anti-aging and skin rejuvenation
- Rationale: Enhances skin firmness, hydration, and antioxidant defense
- Often marketed as “IV beauty drips” or wellness infusions
D. Glutathione + Microneedling (Topical Application Post-Procedure)
- Use: Hyperpigmentation, aging, dull skin
- Rationale: Microneedling enhances transdermal absorption of topical glutathione
- Protocol: Apply GSH serum immediately post-needling
E. Glutathione + Chemical Peels (e.g., Glycolic Acid, Kojic Acid)
- Use: Skin brightening, acne scars, melasma
- Rationale: Peels remove upper pigmented layers; GSH helps prevent rebound pigmentation
F. Glutathione + Laser Therapy (e.g., Q-Switched Nd:YAG)
- Use: Melasma, freckles, uneven skin tone
- Rationale: Laser reduces melanin; GSH maintains even skin tone post-treatment
Summary Table: Aesthetic Protocol Examples
| Goal | Combination | Route |
| Skin lightening | Glutathione + Vitamin C + Oral sunblock | Oral/IV |
| Melasma treatment | Glutathione + Tranexamic Acid + Microneedling | Oral/topical |
| Anti-aging | Glutathione + Collagen + Vitamin C | IV/Oral |
| Post-laser recovery | Glutathione + Hyaluronic Acid serum | Topical |
Hair Transplantation
Module 1: Introduction to Hair Loss & Transplantation
- Definition of alopecia – AGA (androgenetic), alopecia areata, cicatricial, telogen effluvium
- Epidemiology: Common age groups, male vs female prevalence
- Genetic & hormonal basis – Role of DHT (dihydrotestosterone) in AGA
- History of hair transplant – Dr. Norman Orentreich’s work to modern techniques
- Medical vs Surgical treatment – Indications for hair transplant (stable hair loss)
Module 2: Anatomy & Physiology of Hair
- Structure of hair follicle – Shaft, root, bulb, dermal papilla, sebaceous gland
- Hair cycle:
- Anagen (growth): 85-90% of scalp hairs
- Catagen (regression): 1-2%
- Telogen (resting): 10-15%
- Hair follicle types – Terminal vs vellus
- Scalp anatomy: 5 layers (“SCALP”) – Skin, Connective tissue, Aponeurosis, Loose areolar tissue, Pericranium
- Vascular & nerve supply – Important during harvesting
Module 3: Evaluation & Diagnosis
- Trichoscopy – Diagnostic tool to visualize scalp and hair
- Classification systems:
- Norwood-Hamilton scale (Male AGA)
- Ludwig scale (Female AGA)
- Savin scale, BASP classification
- Scalp biopsy indications: To rule out scarring alopecia
- Laboratory work-up: Thyroid function, iron profile, hormonal panel in female patients
- Contraindications: Active scalp infection, unstable alopecia areata, keloid history
Module 4: Transplant Techniques Overview
- FUE (Follicular Unit Extraction)
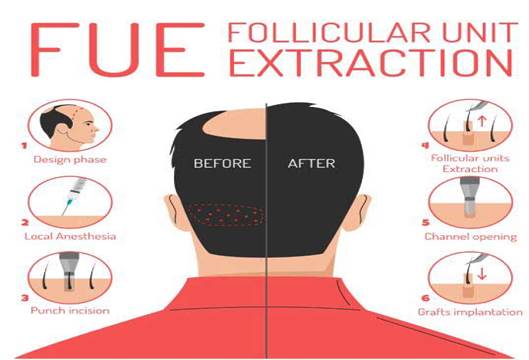
- Principle: Individual extraction of FU with small punch
- Tools: Motorized, manual punches (0.8–1.0 mm)
- Less scarring, faster healing
- FUT (Follicular Unit Transplantation/Strip method)
- Excision of scalp strip from donor
- Slivering under microscope
- Linear scar but more grafts per session
- Modified FUE with immediate implantation via Choi pen
- No need to pre-make slits
- Comparison table: Yield, time, scarring, cost, recovery
Module 5: Donor Area Planning
- Safe donor zone (SDZ): Occipital-parietal area, resistant to DHT
- Donor density assessment: FU/cm² (Normal: 60–100)
- Extraction planning: Avoid overharvesting, maintain natural density
- Punch size selection: 0.8 mm for finer hair, 1 mm for coarse
Module 6: Graft Harvesting
- Depth of punch: Just beyond isthmus
- Follicular transection rate (FTR) – Should be <5%
- Handling grafts: Atraumatic, avoid desiccation
- Slivering (FUT): Use of stereomicroscope to isolate FU
- Storage:
- Mediums: Chilled saline, Ringer’s lactate, HypoThermosol®, PRP
- Temperature: 4°C
- Maximum safe ischemia time: 4–6 hours
Module 7: Recipient Site Creation
- Slit design principles: Direction, angle (30–40°), depth
- Density planning:
- Hairline: 30–40 FU/cm²
- Mid-scalp: 40–60 FU/cm²
- Tools: Slit blades, needles, implanter pens
- Zones: Frontal, temporal, crown, vertex — each has unique orientation
Module 8: Graft Implantation Techniques
- Implantation tools:
- Forceps method
- Sharp/Blunt Choi implanters
- Single vs multiple technician system
- Bleeding control: Adrenaline-soaked gauze
- Graft dehydration risk: Keep moist with chilled saline every 5–10 mins
Module 9: Aesthetic Planning
- Frontal hairline design: “Zig-zag” pattern, avoiding straight line
- Temporal angle design: Acute angles for natural look
- Gender difference:
- Males: M-shaped hairline
- Females: Rounder, lower
- Face proportions: Golden ratio relevance
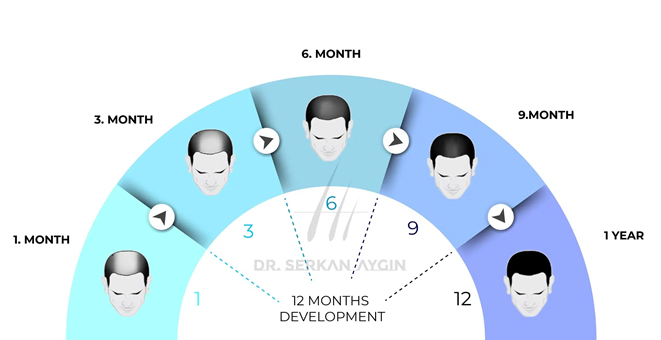
Module 10: Postoperative Management
- First 7 days: Saline spray, antibiotics, avoid head trauma
- 10–15 days: Scab shedding
- 1 month: Shock loss
- 3–4 months: Visible regrowth
- 9–12 months: Final result
- Medications:
- Minoxidil 5%
- Finasteride 1 mg (males only)
- Biotin, multivitamins
- PRP every 30–45 days post-op
Module 11: Complications
- Immediate: Bleeding, pain, dizziness
- Delayed:
- Folliculitis
- Shock loss
- Cobblestoning
- Donor area necrosis
- Pitting/ridging
- Prevention: Proper technique, sterile field, hydration, careful planning
Module 12: PRP & Adjunct Therapies
- PRP (Platelet Rich Plasma):
- Autologous, growth factor rich
- Activates dormant follicles
- Procedure: 15–20 ml blood, centrifugation, scalp injection
- LLLT (Laser therapy):
- 630–660 nm red light
- Improves mitochondrial activity in follicular cells
- Mesotherapy:
- Cocktail of vitamins, minoxidil, peptides
- Oral support: Biotin, zinc, omega-3, saw palmetto
Module 13: Special Indications
- Beard transplant: Male aesthetics, post-trauma
- Eyebrow transplant: Artistic angling
- Scalp scar camouflage: Post burn/trauma
- Transgender care: Gender-affirming hairline design
Module 14: Ethics & Consent
- Consent form components:
- Risks, expectations, number of grafts, anesthesia
- Medical photography consent
- Marketing ethics: No false claims, realistic before-after photos
- Legal considerations: Licensing, trained staff, OT compliance
FACE ACNE SCAR
1. Introduction
Definition:
Acne scars are permanent changes in skin texture or pigmentation following inflammatory acne. Scars result from dermal collagen destruction or excess deposition during healing.
Epidemiology:
- Affects up to 95% of acne patients to varying degrees.
- More prevalent in Fitzpatrick Skin Types IV-VI due to risk of PIH.
2. Pathophysiology of Acne Scarring
Inflammatory Process:
- Inflammatory lesions (papules, pustules, nodules) → dermal injury.
- Neutrophils & cytokines (IL-1, TNF-α) stimulate MMPs.
- Matrix metalloproteinases (MMPs) → collagen breakdown.
Healing Response:
- Insufficient collagen = Atrophic scars
- Excess collagen = Hypertrophic or Keloid scars
- Melanocyte stimulation = PIH
Classification of Acne Scars
A. Atrophic Scars (80–90%)
- Ice Pick Scars
- Deep, narrow, V-shaped (<2 mm)
- Extend into dermis/subcutis
- Most difficult to treat
- Boxcar Scars
- Broad, sharp edges
- U-shaped; can be shallow or deep
- Common on temples and cheeks
- Rolling Scars
- Wavy, shallow depressions with ill-defined borders
- Caused by dermal tethering
B. Hypertrophic & Keloid Scars
- Thick, raised, fibrous tissue
- Extend beyond the original acne lesion (keloid)
- Common over chest, back, jawline
C. Post-Inflammatory Hyperpigmentation (PIH)
- Epidermal PIH – brown color
- Dermal PIH – gray-blue color
- More visible in skin types IV–VI
4. Clinical Evaluation
Assessment Parameters:
- Scar type(s) and extent
- Depth (superficial vs deep)
- Fitzpatrick skin type
- Skin texture and elasticity
- Patient’s psychological concern
Grading Systems:
- Goodman and Baron Scoring System
- ECCA Score (Echelle d’Evaluation Clinique des Cicatrices d’Acné)
5. Treatment Modalities: Overview by Scar Type
| Scar Type | Best Treatments |
| Ice Pick | TCA CROSS, Punch Excision |
| Boxcar | Subcision, Laser, Microneedling |
| Rolling | Subcision, Microneedling, RF |
| Hypertrophic | IL Triamcinolone, Silicone, Laser |
| PIH | Topicals, Chemical Peels, Non-ablative Laser |
6. Advanced Treatment Modalities
A. Laser Resurfacing
- Fractional CO₂ Laser
- Ablative, improves texture and collagen remodeling
- Downtime: 5–7 days
- Er:YAG Laser
- Precision with lower heat damage
B. Microneedling
- Controlled dermal injury via 0.5–2.5 mm needles
- Stimulates neocollagenesis
- Best for rolling scars
- Often combined with PRP (vampire facial)
C. Subcision
- Performed using Nokor or blunt-tipped cannula
- Used for tethered rolling scars
- Combines well with fillers or RF
D. TCA CROSS
- High concentration (70–100%) TCA applied focally
- Induces dermal remodeling
- Best for ice pick scars
E. Punch Excision/Elevation
- Surgical removal or elevation of deep boxcar or ice pick scars
- Requires good wound healing
7. Adjunct Therapies
Dermal Fillers:
- Temporary correction (Hyaluronic Acid)
- Restore volume under atrophic scars
- Duration: 6–12 months
Chemical Peels:
- Superficial: Glycolic, Salicylic, Lactic acids
- Medium: TCA (15–35%)
- Improve pigmentation and superficial scars
Platelet-Rich Plasma (PRP):
- Enhances wound healing
- Stimulates fibroblasts and collagen
- Used with microneedling/lasers
8. Complications & Risk Management
Complications:
- PIH (especially in darker skin)
- Erythema, edema, scabbing
- Infection (bacterial, viral)
- Worsening of scars (over-aggressive treatment)
Prevention:
- Priming with hydroquinone + retinoids before procedures
- Sunscreen post-treatment
- Aseptic technique
9. Case-Based Clinical Discussions
Case 1: Rolling + Boxcar Scars (Type IV Skin)
- Treatment: Subcision + Microneedling RF
- Follow-up: PRP + TCA 20% Peels
- Outcome: 60–70% improvement in texture
Case 2: Ice Pick Scars + PIH (Type V Skin)
- Treatment: TCA CROSS + Topical depigmenting agents
- Complication: Mild PIH – managed with sunscreen & azelaic acid
Case 3: Hypertrophic Scar on Jawline
- Treatment: IL triamcinolone + silicone gel
- Alternative: Pulsed dye laser for erythema
10. Summary
- Accurate scar classification is key to treatment planning.
- Combination therapies yield the best results.
- Always consider patient skin type, tolerance for downtime, and psychological impact.
- Monitor for complications and counsel patients on realistic expectations.
Diploma Course in Aesthetic Dermatology & Skincare
- DAY – 02
- Botox
- Filler
- Thread

BOTULINUM TOXIN
Background Of BOTOX
- Botulinum Toxin is a neurotoxin made by the bacteria Clostridium Botulinum; an anaerobic bacteria found in soil. Botulinum Toxin is purified for clinical and cosmetic use.
- First used in the late 1960’s.
- In patients used for facial spasms and it was then noted that facial wrinkling decreased over time.
- First approved in 2002 by the FDA and has since then been used by medical professionals to inject millions of patients each year to successfully treat wrinkles and facial creases.
Medical Indications
- Blepharospasm – Involuntary spasms of the eyelid muscles causing excessive blinking.
- Idiopathic cervical dystonia (spasmodic torticollis) – Involuntary movements/contractions of the neck muscles.
- Severe Hyperhidrosis – excessive sweating of the armpit which does not respond to antiperspirants.
- Overactive bladder – Leakage of urine due to bladder problems associated with spinal cord injury or multiple sclerosis, not adequately controlled with anticholinergic
medicines.
- Hemifacial spasm, a neuromuscular disorder characterised by unpredictable and involuntary twitching of facial muscles on one side of the face.
- Migraine – BOTOX® is licensed specifically for the treatment of chronic migraine but has not been shown to be effective for any other headache type (e.g., episodic migraine, tension type headache, cluster headache) yet.
Cosmetic Uses
- Glabellar lines (Corrugator Supercilii, Procerus, & Depressor Supercilii)
- Crow’s feet – Orbicularis Oculi
- Forehead lines – Frontalis
- Downturned corners of the mouth
- Excessive sweating
- Correct facial asymmetry
- Bunny lines
- Eyebrow lifting
- Wrinkles caused by sun damage and gravity will not respond to Botox
Product Safety
- Botox has a long clinical history
- Maximum dose per treatment for muscle spasms is 400 units
- Cosmetic doses range between 20 – 80 units
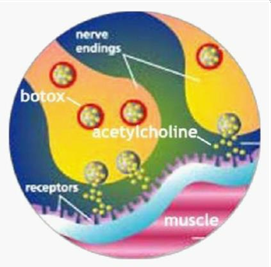
Mechanism Of Action
- Once injected into the muscle, the mechanism of action of botulinum toxin is to cause temporary muscle paralysis through inhibiting the release of the neurotransmitter acetylcholine from motor nerve terminals. This prevents muscular contraction and hence creates the desired cosmetic effects. With time, synaptic-sprouting and receptor formation leads to the reoccurrence of muscular contractions and hence the ‘wearing off effect’ of botulinum toxin.
Fig. 1. Botox effect on muscle nerve terminals
What To Tell Your Patient
- Tiny quantities of the toxin are injected directly into the affected muscles. It takes three to five small injections between the eyebrows to treat frown lines. The injection is almost painless. The treated muscles weaken over the following week or so. Most people do not notice anything. They simply become aware that they are no longer able to contract the frown muscles. They can still lift their eyebrows normally and blink
without problems.
- The effects of Botulinum Toxin start wearing off within 3 months. Some areas may return to activity sooner or later depending on the injection area, muscle strength, who did the injection and amount injected.
- Many people find after three or four treatments to glabellar lines that they don’t need another one for a long time, the muscles have weakened, or they have broken the bad habit that led to the frowning or squinting originally.
The Consultation
- Understand patients desires and preferences
- Avoid dissatisfaction by establishing realistic expectations
- Botox does not erase lines it relaxes them. Deeper lines will become less deep and superficial lines will nearly disappear
- Under inject on the 1st appointment
- Photographs
- Accurate medical history including allergies
- All medication (e.g., blood thinners)
- Future & past surgery
- Assess for weakness of forehead muscles / drooping eyelids
Side Effects
- Mild-temporary headache
- Swelling and bruising (can occur even among the most skilled injector. Take precautions to watch out for vessels or aggressive manoeuvring)
- Tenderness
- Dry eyes / mouth
- Muscle weakness / fatigue / heaviness
Headache and injection-site reactions have been reported as the most common adverse effects.
Cautions & Contradictions
Contraindications for Treatment:
- Those with a known hypersensitivity to Botulinum Toxin Type A or to any of its’
excipients e.g., human albumin, and sodium chloride.
- Neuromuscular disorders such as myasthenia gravis or Eaton Lambert Syndrome.
- Pregnancy or breast feeding.
- Co-treatment with Aminoglycoside antibiotics, or medicinal products which interfere with neuromuscular transmission (e.g., tubocurarine – type muscle relaxants).
- < 18 years old
- Concurrent use of Anticoagulants, Aspirin, Vitamin E, Chloroquine, Calcium antagonists Cautions for Treatment:
- Caution should be used in those with coagulation disorders or using anticoagulants due to the increased likelihood of bruising.
- Caution should also be used in patients with Amyotrophic lateral sclerosis or with peripheral neuromuscular disorders.
Different Brands of Botox
- Botox® Type A, Dysport®, Azzalure®, Xeomin®, Bocouture®.
- 2002 – Allergan earned FDA approval for cosmetic use.
Dilutions of Various Botulinum Toxins
There are many different botulinum toxins available commercially. The three main manufacturers are Allergan, Merz and Galderma. All vials come in powder form which must be reconstituted for injection with 0.9% sodium chloride solution. This process should be done slowly to avoid denaturing the product. Once reconstituted it must be used within a period of 2 weeks, after this it loses efficacy.
Botulinum toxin effects start within 2 weeks and will generally last for around 3 – 4 months. Immunogenicity with botulinum toxin is typically reported when large doses are injected for therapeutic rather than cosmetic reasons. Immunogenicity may be avoided by administering treatment no less than 3 monthly and by avoiding top-up treatments.
The table below outlines the 3 main groups and their respective preparations and dilutions: Botox, Azzalure and Bocouture:
There are a number of product brands under the different Botulinum toxin A subtypes listed above:
| Type of Botulinum Toxin A | Saline Reconstitution | Units per 0.1ml |
| Allergan Botox 50 Units | 1.25ml | 4 units |
| Allergan Botox 100 Units | 2.5ml | 4 units |
| Bocouture 50 Units | 1.25ml | 4 units |
| Bocouture 100 Units | 2.5ml | 4 units |
| Azzalure 125 SU | 0.63ml | 20 SU |
Practitioners may inject botulinum toxin with differing dilutions, different angles and different injection techniques which is acceptable however each product will have specific manufacturer guidelines regarding dilution, dosing and injection sites. Botox is typically diluted with 2.5ml per 100 units of normal saline. Azzalure 125 SU is typically diluted with 0.63ml saline giving a concentration of 10SU/0.05mls.
Patient Positioning
Positioning the Patient
The most commonly used and ideal position to administer treatment is to have the client sitting upright between 60 and 90 degrees. The reason for this is twofold:
- To be on a similar level and dimension to the injector
- To identify gravitational effects which may influence treatments.
Equipment
Equipment needed for diluting and administering toxin treatments the following are needed:
- 1ml syringe
- Green 21 gauge needle (1.5 inch) for dilution
- Yellow 30 gauge needle (1/2 inch) for injection
- Antiseptic/sterile wipes
- Gauze pads
- Sharps bin
Injection Precautions
- Always wash hands and glove-up prior to injecting
- Make sure the scale on the syringe is visible to monitor dosage
- Be aware of needle depth and angle of injection in certain areas
- Always inject away from key structures like the orbit and vessels
- Mark out landmarks prior to injection according to your client’s anatomy
Treatment areas
Knowledge of the relevant facial anatomy is pertinent prior to administering treatments:
Preparation
- Wash hands.
- Disposable gloves/apron.
- Sharps Bin.
- Headband.
- White marking pencil.
- Syringes.
- Alcohol wipes.
- Bacteriostatic saline.
- Emergency equipment.
Reconstitution
- Key Points: avoid bubbles, avoid forcing saline into vial, draw up slowly.
- Botox has to be stored in fridge. (2-8 degrees)
- Make sure vial is sealed before opening.
- Check expiry date.
- Remove lid.
- Put the green needle in the middle of vial – listen to the hiss.
- Withdraw 1.25mls – get rid of air.
- Ensure no bubbles.
- Rotate vial gently to mix until clear liquid – do not shake.
- Prime needle right to the end.
The Procedure (Cleansing)
- Head band to facilitate exposure.
- Skin preparation, clean skin with alcohol wipes.
- Wipe away from injecting area.
- Ensure no oil moisturizers.
- Apply Emla topically if needle phobic. (rub off after 15mins)
The Procedure (Marking)
- Assess & mark the face even if you are experienced – good practice takes time.
- Contract the muscles and note where the wrinkles are forming.
- Use the white pencil to mark the intended injection sites.
- Procerus – should ideally be in the middle of the eyebrows.
- Corrugator – bulge above the eye. Mark out mid pupillary line do not inject lateral to this point! Avoid ptosis & brow drop.
- Frontalis – bear in mind the muscle runs vertical so therefore do not mark in the triangle. In females we tend to inject in a V pattern. (Sometimes wrinkle go into the hair line so be mindful and mark). Do not inject within 1cm of the brows.
- Periorbital – feel orbital rim in line with the lateral campus of eye. Mark 1cm from it, with superior and inferior boarders.
Muscles
- 1st Procerus – contracts and creates frown. Pinch muscle for improved accuracy. Inject directly into the muscle.
- 2nd Corrugator Supercilii – lifts and separates – long muscle requires two injections. Pinch muscle and inject away from eye.
- 3rd Frontalis – thinner so don’t need to go as far in – requires 5 injections – lifts upwards therefore Botox relaxes. It can cause a big problem if it is not done correctly.
- 4th Orbicularis Oculi – crow’s feet (3 injections – vascular therefore higher risk of bruising).
- 5th Depressor Supercilii – bunny lines.
The Most Popular Treatment Areas:
Glabellar / Frown Lines
- Treatment of vertical glabellar frown lines is perhaps the most commonly administered BOTOX® treatment. Vertical frown lines form in the glabellar area after repeated frowning caused variously by expressions of disapproval, anxiety, and anger.
- Primary muscles: Corrugator Supercilii, Procerus, Depressor Supercilii.
Frontalis / Forehead Lines
- This muscle group works to pull the eyebrows up.
- Before & After
Orbicularis Oculi / Crows Feet
- This muscle is made up of a dual series of concentric curves. The Palpebral part surrounds the circumference of the orbit and spreads over the temple. The Orbital part blends with Frontalis and Corrugator. Together these curves screw the eye shut and pull down the eyebrow.
- Before & After
Allergan and Bocouture Dosages
Recommended Botulinum Toxin Dosages
Gender Differences
- Gender importance, due to men having larger muscle mass.
- Shape of male brow is horizontal, and females is a gentle arch.
- In studies most used is 20-30 units in the glabella for women.
- Men frequently required larger doses.
- Thicker sebaceous skin requires higher doses.
Complications and Management
Brow Ptosis – Often the result of injecting into the wrong muscle group (Frontalis) within the danger zones. Cannot be corrected, must allow natural Resolution.
Eyelid Ptosis – Often results from injecting to close to the palpebral part of the Orbicularis Oculi. Can either allow natural resolution (usually 2-6 weeks), or consider Iopidine (Alcon) eye drops three times a day until resolution
Spock Eyes – ‘SPOCK EYEBROWS’ – often a result too few Lateral frontalis injections. Ask your client to raise eyebrows and inject a small amount (1-2 units), 1.5- 2cm above the frontalis pull.
Forehead Heaviness – often a result of injecting too low. In future maintain injection sites higher.
Post Treatment Advice & Reviews
It is good practice to review all patients 2 weeks after treatment. Firstly, you will learn from your work, and secondly, you will gain an understanding of what works for each patient you treat. Reviews are generally free of charge and enable you to ‘top-up’ if an unsatisfactory outcome is achieved. Should top-up treatments of botulinum toxin be required, often the same dosage or half the original dosage is required. This should be accurately documented for future use.
Aftercare Advice:
- Avoid high intensity exercise immediately following treatment for 24hrs
- Avoid touching/rubbing areas injected
- Avoid heavy alcohol consumption on same day
- Remain upright for at least 3hrs afterwards
- Exercise injected muscles
- Full effect will be at around 2 weeks
- Duration of action ~3 months
Causes of Treatment Failure Include:
- Incorrectly placed toxin
- Suboptimal dose (offer a top-up either at a lower dose or consider original dose again)
- Inactivated toxin due to poor storage
- Resistance due to blocking antibodies
Advanced Botulinum Toxin Procedures
Hyperhidrosis (Excessive Sweating)
Superficial dermal injections into apocrine sweat glands preventing sweat production. This doesn’t cure hyperhidrosis but provides temporary relief and needs to be repeated every five to six months for maximum effect.
- Landmarks: Draw around hair follicles, create 20 injection sites.
- Dose: 2 units in each injection site, 40 units per axilla, 80 units per patient.
- Onset: With 1 week.
- Duration: 4-6 months.
Massater Muscle
Botox is injected into the ‘chewing’ muscles of the jaw (called the massater muscle) to
reduce its size.
- Landmarks: Into thickened masseter below the ear (palpate the masseter by asking patient to clench their teeth then relax). Draw 4 compartments, injecting the centre of each – insert 1⁄2 to 2/3rd of needle at 90°
- Dose: 4 injections of 4 units, 32 units in total – top up in 4 weeks with half the dose.
- Onset: 4-6 weeks
- Duration: 4-6 months
Brow Lift
- Landmarks: tail of brow, into Orbicularis Oculi (Superficial 20°injection into the upper part of the orbicularis oculi, 1cm from orbital rim)
- Dose: 1 injection of 2 units, 4 Units in total – top up in 2 weeks with same dose.
- Onset: 2 weeks.
- Duration: 3-4 months.
It is important to point the injection needle superiorly to avoid downward dispersement of the Botox.
Bunny Lines
- Landmarks: each side of nasal bridge – superficial 90° injection either side of the while the patient is asked to contract the muscle.
- Dose: 1 injection of 2 units each side, 4 units in total – top up in 2 weeks with same dose.
- Onset: 2 weeks
Gummy Smile
A gummy smile is usually caused by an overactive upper lip muscle that lifts the lip too high when smiling, revealing too much of the gum line
- Landmarks: both nasal alar triangles. 90° injection, half the needle in the middle of triangle
- Dose: 1 injection of 2 units each side, 4 units in total – top up in 2 weeks with same dose or half the dose
- Onset: 2 weeks.
- Duration: 3-4 months.
- Nicely combined with lip fillers.
- Patients should be told that they may feel funny when smiling, whistling, and sometimes eating as the lack of movement can come as quite a surprise to some of them.
Caution must be taken as excessive Botox in the lower face may have very obvious cosmetic and functional impairment. It is very important to start conservatively when treating this area – you can always add more if needed.
Down Turned Mouth
Depressor Anguli Oris (DAO): pulls down corners of mouth (while Zygomaticus pulls up). A
small amount of Botox into the DAO muscle can diminish the downward pull on the corners of the mouth and allow the muscles that elevate the corners to take over hence subtly lifting the corners of the mouth.
Identified by asking patient to show lower teeth or look upset → creates ‘dimple’.
- Landmarks: 1 injection site below each oral commissure – draw line from oral
commissure to jawline. Inject halfway between them (into dimple) inserting half the needle at 90° angle.
- Dose: 2 injections of 2 units, 4 units in total – top up in 2 weeks with same dose
- Onset: 2 weeks
- Duration: 3-4 months
Pebble Dimpled Chin / Mentalis
Mentalis: repeated contractions can cause ‘dimpling’ – Botox relaxes and smoothens the chin & mental crease.
- Landmarks: 2 injections 1cm apart at the bottom / central of chin.
- Dose: 2 injections of 2 units, 4 units in total – top up in 2 weeks with same dose.
- Onset: 2 weeks.
- Duration: 3-4 months.
- To identify this muscle, ask patient to ‘pout’ or lift up the lower lip. Place index finger in
the middle of chin, pinch the muscle and insert half the needle at 90° angle.
Smokers Lines aka Perioral Lines / Orbicularis Oris
Smokers/perioral radial lines are fine wrinkles and lines on the upper and/or lower lip that are caused by the contraction of the Orbicularis Oris muscle that surrounds the mouth.
Perioral radial lines can be treated in a number of ways. If the lines are early in their development and are visible only when the perioral muscles contract and purse the lips, relaxation of the perioral muscles with Botox can be used,
· Landmarks:
- Botox: 4 injections 5mm above VB, injected at 90 degrees at a depth of about 2 mm
- Filler: superficial, 5mm above VB, linear threads injected parallel to the vermilion border, at a depth of 1-2 mm.
o Don’t inject into philtrum
- Dose: 4 injections of 1 unit, 4 units in total – top up in 2 weeks with same dose.
- Onset: 2 weeks.
- Duration: 3-4 months.
Neck Botox / Platysmal Bands & The Nerfertiti Lift
This is a new technique which involves placing multiple injections of Botox horizontally along the lower jawline and vertically down the side of the neck along the platysmal band muscles.
- Landmarks: either side of trachea → trapezius.
- Dose: 24 injections of 2 units, 48 units in total.
- Onset: 4 weeks.
- Duration: 4 months.
Tips
- Every action has a reaction.
- Professional environment.
- Good lighting.
- No bubbles.
- Beware superficial veins especially for crow’s feet injections.
- Always use white pencil for markings.
- Practice taking photos.
- Be safe – avoid needle stick injury.
Obtaining Botox
- Botulinum Toxin is a prescription only medicine (POM) which means that it has to be prescribed by an authorised health care professional (e.g., doctors, dentists, nurse prescribers that have trained in the administration of botulinum toxin) and has to be dispensed from a pharmacy.
- If you are a non-prescribing practitioner, you will need to use either a prescribing service or buddy up with a local prescriber in order to obtain a prescription for Botulinum Toxin. Your prescriber will need to complete an initial face to face
consultation with the patient before writing the prescription, but they do not need to be present when you administer it.
- After obtained a prescription for Botulinum Toxin, you will need to order the product. Your prescriber might order it on your behalf. Have it sent out to you or order it yourself through an online pharmacy. Your prescriber will have to electronically sign the prescription before the transaction is approved.
Safety & Infection Control
Injectable treatments provide a direct route for infectious pathogens to enter the
circulatory system and puts the practitioner at risk of exposure to the patient’s blood.
Always assume that all “blood and body fluids” are infectious for blood-borne diseases such as HIV, Hepatitis B and Hepatitis C.
The following standard infection control precautions help reduce the risk of healthcare acquired infections.
· Hand hygiene
- Good hand hygiene is the single most important way of preventing the spread of infection. Hand hygiene describes processes that reduce the number of micro-organisms and includes hand washing and use of alcohol gel. Effective hand hygiene involves making sure all aspects of the hands have been cleaned
- If hands are visibly soiled or potentially contaminated wash hands with antibacterial soap and water and dry with single use towels
- If hands are not visibly contaminated, clean with alcohol rub
- To support compliance with hand hygiene in the workplace, practitioners should meet the following standards while working:
- keep nails short, clean and polish free
- avoid wearing wrist watches and jewellery
- avoid wearing rings with ridges or stones (a plain wedding band is usually acceptable)
- cover any cuts and abrasions with a waterproof dressing
- wear short sleeves or roll up sleeves prior to hand hygiene
- To support compliance with hand hygiene in the workplace, practitioners should meet the following standards while working:
· Personal Protective Equipment (PPE)
- Standard infection control precautions advise that practitioners should wear protective clothing appropriate to the clinical activity.
· Gloves
- Practitioners should wear well fitting, non-sterile gloves when taking blood (gloves should be close fitting otherwise dexterity will be impaired). Practitioners should also carry out hand hygiene before and after each patient procedure (use one pair of gloves per procedure or patient).
- Natural latex rubber (NLR) proteins found in latex gloves can cause severe allergic reactions – following a risk assessment, if latex gloves are selected, they must be low protein. Neoprene or nitrile are good alternatives to NLR showing comparable barrier performance.
· Skin cleansing
- The use of an appropriate skin disinfectant will reduce the number of micro- organisms at the site of insertion.
- Skin cleansing with 2% chlorhexidine in 70% isopropyl alcohol is recommended. Chlorhexidine is an anti-microbial agent that has been shown to reduce the risk of infection.
- Clean the site for 30 seconds and allow to dry completely (30 seconds).
· Sharps disposal
- To minimise the risk of injury, sharps should never be re-sheathed and should be discarded into an appropriate sharps bin immediately after removal from the patient. Place the sharps bin within easy reach, no more than one arms distance away from the client. They should not be filled above two-thirds full (there is a mark on the side indicating the fill line).
Needlestick Injuries
A needlestick injury is an incident in which the needle penetrates the skin. Needles
contaminated with infected patient’s blood can transmit up to 20 types of diseases including hepatitis B, hepatitis C and HIV. Needle stick injuries occur due to poor technique or inappropriate handling of needle. Any accident no matter how minor it may seem should be documented, reported to the manager, and receive medical attention.
If you sustain a needlestick injury, follow this process immediately:
- Remove your gloves and dispose of them carefully
- Gently squeeze the wound to encourage it to bleed
- Wash the wound using running water and plenty of soap
- Don’t scrub the wound while you are washing it
- Don’t suck the wound
- Dry the wound and cover it with a waterproof plaster or dressing
You should then attend the nearest A&E department or contact a local sexual health clinic for a blood test.
The healthcare professional treating you will assess the risks to your health and ask you about your injury. Samples of your blood may be tested for Hepatitis B, Hepatitis C or HIV. Your healthcare professional may also arrange to test samples of the other person’s blood if they give their consent.
If you are deemed to be at low risk, you may not need any treatment. If there’s a higher risk, you may need:
- Antibiotic treatment
- Further vaccination against Hepatitis B
Avoid a needle stick injury at all cost by good practice when dealing with sharps and remaining vigilant throughout all procedures
Practitioners undertaking injectable treatments should be vaccinated against hepatitis B
Medical Emergencies
Anaphylaxis – a severe and potentially life-threatening reaction. Signs and symptoms:
- Feeling light headed or fainting
- Constriction of airways – breathing difficulties and wheezing
- Fast heartbeat
- Low blood pressure
- Skin reactions e.g., hives
- Nausea or vomiting
See Appendix 1 for the treatment of acute anaphylactic reaction See Appendix 2 for Adult Basic Life Support (BLS)
Necrosis – death of body tissues usually due to a failure of blood supply Signs and symptoms usually occur simultaneously with the injection.
- Pain
- Prolonged blanching of the skin
- Skin discolouration – purple indicates tissue death
- Numbness and coolness of the skin.
Accreditation Registers – Save Face and JCCP
Businesses offering cosmetic procedures are subject to a wide range of laws and duties. These primarily relate to public health, occupational health and safety, environmental protection, and in some parts of the UK to public control licensing. Most of this law is administered by local authorities, often through their environmental health departments.
It was suggested in the Keogh review that restrictions should be applied to the types of premises used to deliver treatments where clinical oversight was requested, for example, clinics equipped to deal with medical emergencies. It has been left up to the individual providing clinical oversight to ensure the provision of an appropriate and safe environment. Hygiene measures, sharps disposal, in-date products and safety equipment are a must for all situations regardless of venue choice and will be taught during the practical training days.
Save Face
Save Face Ltd is an independent and impartial accreditation scheme for aesthetic medical professionals and clinics. They offer an optional registration service to regulated health professionals only and audit practitioners against seven core standards. Each practitioner must supply:
- Evidence of registration and qualification with the relevant statutory board.
- Evidence of insurance and training for each procedure offered
- Evidence of mandatory training
- Evidence of registration with The Information Commissioners Office
- Samples of patient information
- Consent forms
- Evidence of legitimate supply of medicines
Each clinic premise is inspected by auditors who ensure standards are met with regards to infection control, consent and confidentiality, management and reporting of adverse events, appropriate sharps disposal, record keeping, managing complaints and quality of equipment.
A breach of standards can result in investigation, suspension, or exclusion from the Save Face Ltd register. As this register gains momentum and reputation, clients/patients will increasingly look for such quality standard verification.
Joint Council for Cosmetic Practitioners (JCCP)
The JCCP has been established to assist members of the public who are seeking/considering or undergoing non-surgical and hair restoration treatments (Injections, Fillers, Lasers, Peels and Hair Restoration) with advice on patient safety matters and how to gain access to registers of approved practitioners
The JCCP Practitioner Register has been established to enable practitioners delivering the aesthetic treatments set out in the CPSA Framework of Standards and Competences to be accredited.
- In order to be accredited applicants will need to demonstrate evidence of competence and proficiency.
- The JCCP recognizes that different practitioners will have varying levels of experience, qualifications, and status.
- The public will be able to access the JCCP Practitioner Register and see at what level and which areas of treatment a practitioner has been accredited by the JCCP.
The JCCP Practitioner Register is voluntary and remains subject to consideration
for approval by the Professional Standards Authority (PSA) who oversee public registers in the health care sector.
APPENDIX 1. Treatment of acute anaphylactic reaction (Resus council protocol UK)
APPENDIX 2. Adult Basic Life Support (BLS)
APPENDIX 3. Botox Placement
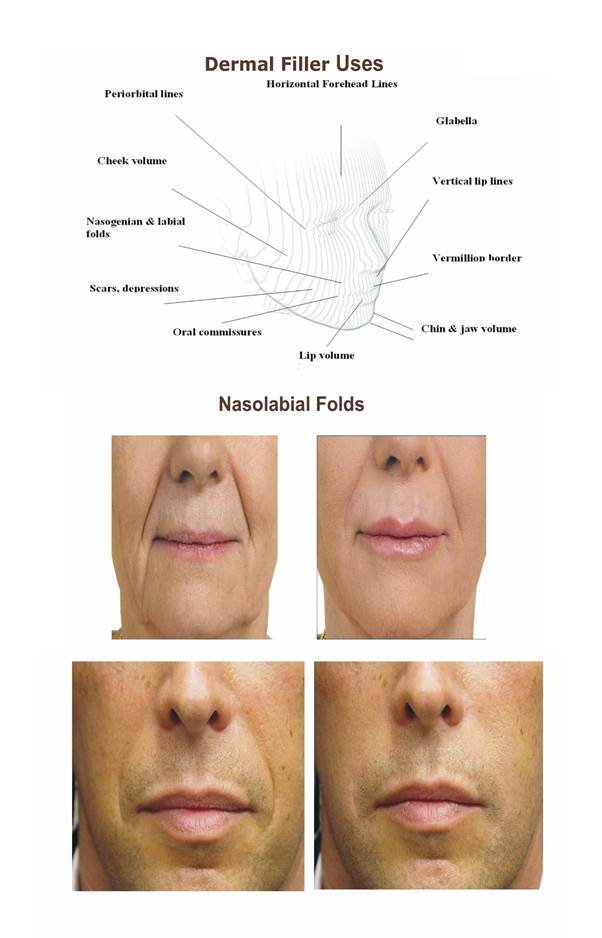
Dermal Filler

THREAD
PART 1: Introduction
Definition:
Thread lifting is a minimally invasive cosmetic procedure where temporary sutures (threads) are used to lift and reposition sagging skin, and stimulate collagen production for rejuvenation.
Historical Evolution:
- Early threads: Permanent, non-absorbable (e.g., polypropylene)
- Modern threads: Biodegradable, absorbable materials (e.g., PDO, PLLA, PCL)
Types of Threads:
| Thread Type | Material | Duration | Example Use |
| PDO (Polydioxanone) | Absorbable | 6–9 months | Common for facial lift |
| PLLA (Poly-L-lactic acid) | Absorbable | 12–18 months | Longer collagen effect |
| PCL (Polycaprolactone) | Absorbable | Up to 24 months | Longest collagen support |
PART 2: Anatomy & Physiology Relevant to Threads
Target Skin Layers:
- Threads are typically placed in the subdermal or SMAS layer.
- Avoid major blood vessels, nerves, and fat compartments.
Mechanism of Action:
- Mechanical lifting by anchoring and pulling sagging tissue.
- Collagen stimulation: Threads trigger a wound-healing response → neocollagenesis → improved firmness and elasticity.
Key Facial Danger Zones:
- Infraorbital foramen
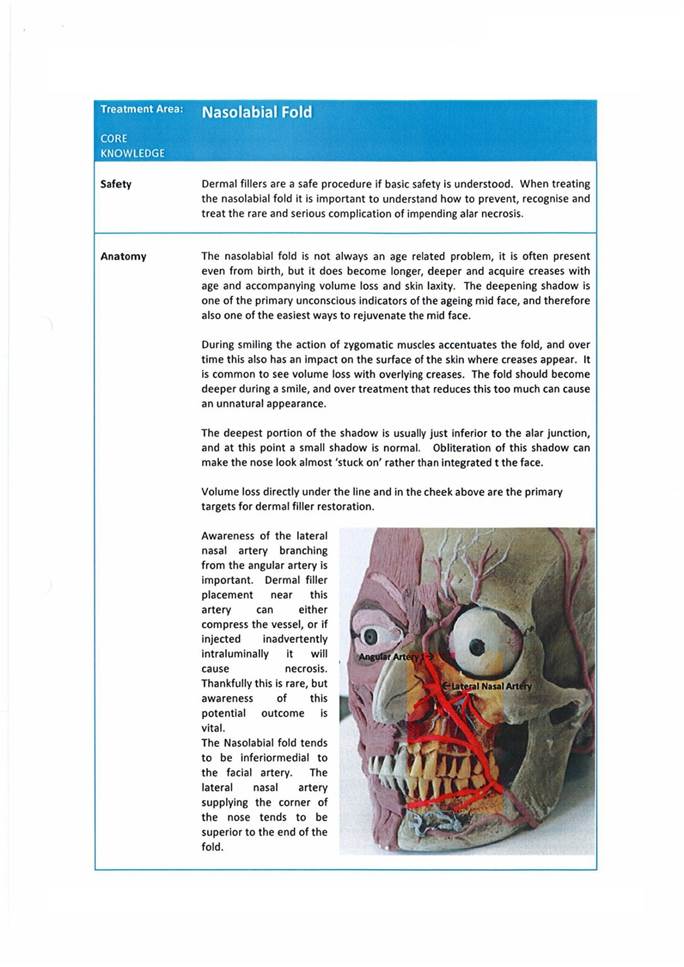
- Facial artery (near nasolabial fold)
- Temporal branch of facial nerve
PART 3: Indications & Applications
Aesthetic Indications:
| Area | Effect |
| Midface (cheeks) | Lifting and volume restoration |
| Jawline (jowls) | Definition and tightening |
| Neck | Skin tightening |
| Eyebrow lift | Brow elevation |
| Nasolabial folds | Softening of deep lines |
| Marionette lines | Reduction of downward pull |
| Nose bridge and tip | Non-surgical nose lift |
Medical Use:
- Facial asymmetry correction (post-stroke or palsy)
- Support in skin ptosis from weight loss or aging
PART 4: Patient Selection & Assessment
Ideal Candidate:
- Age 30–55 with mild to moderate skin laxity
- Not ready for surgical facelift
- Good skin thickness and elasticity
- Realistic expectations
Contraindications:
- Severe skin laxity (surgical candidates)
- Active skin infections or inflammation
- Autoimmune disease or poor wound healing
- Pregnancy or breastfeeding
- History of keloid scarring
Pre-Treatment Workup:
- Facial analysis: symmetry, skin thickness, laxity zones
- Mark key vectors for thread insertion
- Obtain informed consent
- Photographic documentation
PART 5: Injection Techniques & Dosage
A. Types of Threads by Design:
| Thread Design | Action |
| Mono threads | Collagen stimulation, skin texture |
| Cog/barbed threads | Lifting effect via mechanical traction |
| Screw/twin threads | Volume enhancement in hollows |
B. Insertion Technique Overview:
- Marking: Determine lifting vectors
- Antisepsis: Clean face with antiseptic
- Anesthesia: Local anesthesia with lidocaine
- Cannula/Needle Insertion:
- Threads introduced using cannula (blunt tip) or needle (sharp tip)
- Depth: Subcutaneous or SMAS layer
- Position & Anchor:
- Gently pull threads upward
- Anchor barbs in tissue
- Cut Excess Thread: At skin entry
Sample Dosage / Thread Count:
| Area | Type | Typical Threads |
| Cheeks | Cog / barbed | 2–4 per side |
| Jawline | Cog | 2–4 per side |
| Eyebrows | Mono/cog | 1–2 per brow |
| Nasolabial folds | Screw / mono | 3–5 per side |
PART 6: Managing Complications & Side Effects
Common Side Effects:
| Issue | Management |
| Bruising or swelling | Cold compress, resolves in days |
| Discomfort or tightness | Analgesics |
| Dimples or puckering | Usually resolves in 1–2 weeks |
| Mild asymmetry | Observe; minor corrections later |
Major Complications:
| Complication | Cause | Management |
| Infection | Poor aseptic technique | Antibiotics, removal if necessary |
| Thread extrusion | Superficial placement | Trim or remove thread |
| Nerve injury | Incorrect plane or depth | Observation, refer neurology |
| Hematoma | Vessel injury | Compression, drainage if needed |
| Skin necrosis (rare) | Vascular compromise | Immediate care, stop procedure |
Post-Procedure Care:
- Avoid facial massages, dental work for 2 weeks
- Sleep face-up for 3–5 nights
- Limit exercise for 48–72 hrs
- Avoid alcohol and smoking
Summary for MBBS Students
- Thread lifting is a non-surgical option for facial rejuvenation and lifting.
- Knowledge of anatomical layers and vascular danger zones is critical.
- Technique varies depending on thread type, insertion plane, and desired result.
- Requires a safe, sterile environment, and proper patient evaluation.
- Emergency preparedness for complications like vascular injury or infection is vital.
Leave a Reply