
Advance Diploma Course in Aesthetic Dermatology & Sexology
Course Duration : 2 Days
Course Target : Aesthetic Dermatology & Sexology
Faculty : Dr. Refazul Alam (refat) , Dr. Syeda Maria Adnin / Dr. Afnan H Tanna, Dr. Jinat Khan / Dr. Nizhum Ahmed & Dr. Masuma Munni
Open to All MBBS Students undergoing Internship , MBBS & BDS.
CPD certificate in Advance Diploma Aesthetic Dermatology & Skincare will be awarded.
| DAY 1: 5th July 2025 (Saturday) Skin Anatomy of Genital & Intimate Areas, Hyperpigmentation, Laxity & Dermatoses – Diagnosis & Treatment. | |
| 09:15 – 09:30 | Collection of Lecture Course Notes |
| 09:30 – 11:30 | Introduction to conclusion of Skin Anatomy of Genital & Intimate Areas. |
| 11:30 – 11:45 | Morning Tea Break |
| 11:45 – 01:30 | Hyperpigmentation, Laxity & Dermatoses – Diagnosis & Treatment |
| 01:30 – 02.00 | Multiple Choice Question Quiz on Skin Anatomy of Genital & Intimate Areas & Hyperpigmentation, Laxity & Dermatoses |
| 02:00 – 02:30 | Lunch Break |
| 03:00 – 17:30 | Clinical Case Discussion: Vulvar melanosis, Lichen sclerosus, Frictional pigmentation |
| DAY 2: 6th July 2025 (Sunday) Clinical Sexology for both Male & Female | |
| 09:15 – 09:30 | Collection of Lecture Course Notes |
| 09:30 – 10:15 | Details in Clinical Sexology – Sexual Dysfunction & Male & Female Sexual Dysfunctions – ED, PE, Low Libido, Vaginal Dryness |
| 10:15 – 10:30 | Morning Tea Break |
| 10:30 – 12:15 | Advanced Therapy Session: Hormone Balancing, PRP, O-Shot, P-Shot Workshop: Role of Cosmeceuticals & Nutra-pharma in Sexual Wellness Live Roleplay/Case Management: Counseling + Rx + Aesthetic Protocol |
| 12:15 – 12:30 | Multiple Choice Question Quiz on above topic |
| 12:30 – 13:30 | Lunch Break |
| 13:30 – 17:00 | Live Demonstrations and Hands-On Training Workshops Emfemme & Shockwave |
Advance Diploma Course in Aesthetic Dermatology & Sexology
Day 01
- Skin Anatomomy of Genital & Intimate Areas
- Hyperpigmentation, Laxity & Dermatoses – Diagnosis & Treatment
- Clinical Case Discussion : Vulvar Melanosis, Lichen Sclerosus, Frictional Pigmentation
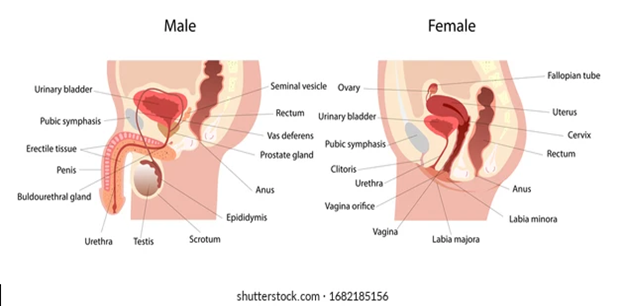
1. General Overview: Regions Considered “Intimate” in Aesthetics
A. In Females
- Mons pubis
- Labia majora
- Labia minora
- Clitoris
- Vestibule & vaginal introitus
- Perineum
- Perianal region
- Inner thighs (considered aesthetically in pigmentation concerns)
B. In Males
- Pubic area
- Penile shaft & glans
- Scrotum
- Perineum
- Perianal region
- Inner thighs
2. Skin Structure in Genital & Intimate Areas
| Layer | Description |
| Epidermis | Thin and delicate, especially in labia minora and glans penis. Keratinized in external structures like labia majora and penile shaft. |
| Dermis | Contains loosely organized collagen and elastin; highly vascularized and innervated. |
| Subcutaneous tissue | Contains fat in mons pubis, labia majora, and scrotum. Thin or absent in labia minora and penis. |
Clinical Notes:
- Thinner skin in these regions means higher absorption of topical agents → caution with acids/retinoids.
- Highly sensitive to hormonal changes, aging, friction, and trauma.
- Prone to post-inflammatory hyperpigmentation (PIH) and chronic dermatoses.
3. Specialized Features of Genital Skin
A. Pigmentation
- Intimate areas are naturally more pigmented due to higher melanocyte density.
- Hormonal influences (estrogen, progesterone) can further increase pigmentation.
- Fitzpatrick IV–VI skin types are more prone to visible darkening.
B. Hair Follicles
- Found in labia majora, mons pubis, scrotum, and pubic region.
- Absent in labia minora, clitoris, glans penis.
C. Sebaceous Glands
- Prominent in non-hair-bearing areas like the inner labia, glans, and foreskin.
- These glands can form Fordyce spots—normal but often mistaken as pathology.
D. Sweat Glands
- Both eccrine and apocrine glands are present.
- Apocrine glands are responsible for body odor and hidradenitis suppurativa.
E. Nerve Supply
- Extremely rich innervation → high sensitivity to touch and pain.
- Important for aesthetic procedures like PRP or laser: require effective topical anesthesia.
4. Male vs Female Genital Skin Differences
| Feature | Female | Male |
| Hair Distribution | Mons pubis, labia majora | Pubis, scrotum, penile shaft |
| Pigmentation | Increases with age, hormonal changes | Often uniform, mild increase with age |
| Laxity Changes | Post-childbirth, menopause | Aging, weight fluctuation |
| Sensitivity | High (clitoris, labia minora) | High (glans, frenulum) |
5. Clinical Relevance in Aesthetic Medicine
A. Why Know the Anatomy
- Prevent complications during lasers, microneedling, PRP, peels
- Ensure accurate depth during filler or PRP injections
- Know the safe vs risky zones (vascularity, nerve density)
- Understand how hormonal changes or trauma affect skin quality
- Design safe & ethical treatments in sensitive areas
6. Aesthetic Implications & Treatments Involving Genital Skin
| Concern | Procedure |
| Hyperpigmentation | Low-fluence laser toning, peels, PRP |
| Laxity/Dryness | RF tightening, laser rejuvenation, PRP |
| Texture Improvement | Microneedling, CO2 fractional laser |
| Scar Correction | Subcision, PRP, laser |
| Hair Removal | Laser hair reduction (caution in skin types IV–VI) |
7. Safety & Ethical Considerations
- Always obtain informed written consent.
- Discuss realistic outcomes and treatment limitations.
- Respect cultural and personal sensitivities.
- Maintain strict hygiene and infection control.
Hyperpigmentation
1. Types of Genital & Intimate Hyperpigmentation
| Type | Description |
| Physiological | Normal darker tone of genitalia due to high melanocyte activity |
| Post-inflammatory (PIH) | After infections, dermatitis, waxing, shaving |
| Hormonal | PCOS, pregnancy, menopause |
| Frictional | Obesity, tight clothing, physical activity |
| Melanosis | Benign pigmented macules on vulva or scrotum |
| Drug-induced | Oral contraceptives, minocycline |
2. Clinical Evaluation
- History: Onset, triggers, trauma, cosmetic use
- Physical exam: Symmetry, color, texture, margins
- Dermoscopy: To rule out melanoma or melanocytic lesions
- Wood’s lamp: To detect depth (epidermal vs dermal pigmentation)
- Biopsy: Rare, unless suspecting malignancy
3. Treatment of Hyperpigmentation
A. Topical Agents (use with caution in genital area):
- Depigmenting agents:
- Kojic acid (1–2%)
- Arbutin
- Azelaic acid (10–20%)
- Niacinamide (2–5%)
- Glycolic acid (very low % only)
- Mild retinoids: Tretinoin 0.025% (not for mucosa, limit use)
B. Chemical Peels (performed by trained aesthetic physicians):
- Mandelic acid 20–30%
- Lactic acid 10–30%
- TCA 10% (only on outer labia/pubic skin; NOT mucosa)
C. Laser Treatments:
- Q-switched Nd:YAG 1064 nm (low fluence): Toning effect
- 4–6 sessions at 3–4 week intervals
D. PRP + Microneedling:
- Safe for pigmentation and rejuvenation
- Enhances melanocyte regulation and skin remodeling
E. Lifestyle & Preventive Measures:
- Weight reduction
- Loose cotton clothing
- Avoid friction, shaving, harsh soaps
SECTION B: Laxity of Intimate Areas
1. Causes of Genital Laxity
- Vaginal childbirth
- Aging (collagen degradation)
- Hormonal decline (menopause)
- Weight fluctuations
- Pelvic floor weakness
2. Clinical Assessment
- Subjective complaints: “looseness,” dryness, decreased sensation
- Physical examination
- Vaginal laxity questionnaires
- Gynecological evaluation if prolapse suspected
3. Treatment Modalities
A. Non-Surgical Aesthetic Treatments
| Procedure | Mechanism | Frequency |
| Fractional CO2 or Er:YAG Laser | Stimulates neocollagenesis & tightening | Monthly x 3 |
| Radiofrequency (RF) | Heats dermis → collagen remodeling | Weekly x 4–6 |
| High-Intensity Focused Ultrasound (HIFU) | Deep tightening | Once every 3–6 months |
| PRP (Platelet-Rich Plasma) | Stimulates fibroblasts, neovascularization | Monthly x 3–4 |
| Microneedling + RF or PRP | Combined tightening + collagen remodeling | Monthly |
B. Adjunctive Measures
- Vaginal moisturizers & lubricants
- Pelvic floor physiotherapy (Kegel exercises)
- Estrogen creams (in postmenopausal women – gynecology-supervised)
SECTION C: Dermatoses of Intimate Skin
1. Common Conditions
| Disease | Features | Diagnosis | Treatment |
| Lichen Sclerosus | White, thin plaques, itching, fissures | Clinical ± biopsy | Topical clobetasol, PRP |
| Lichen Planus | Purplish erosions, painful ulcers | Clinical ± histopathology | Topical steroids, Tacrolimus |
| Frictional Dermatitis | Redness, burning, hyperpigmentation | History + exam | Barrier creams, antifungals |
| Candidiasis | White curd-like discharge, erythema | KOH smear | Fluconazole, topical antifungals |
| Vulvar Melanosis | Flat brown macules, asymptomatic | Dermoscopy | Cosmetic laser if desired |
| Hidradenitis Suppurativa | Recurrent boils, sinus tracts | Clinical staging | Antibiotics, surgery, laser |
| Contact Dermatitis | Itching, redness after products | Patch testing | Discontinue agent, topical steroid |
2. Diagnosis Tips
- Examine under good lighting with privacy & consent
- Dermoscopy can help rule out neoplastic conditions
- Use biopsy selectively (e.g., if melanoma or VIN suspected)
- Consider STD screen in persistent ulcerations
3. Treatment Principles
- Gentle cleansing: pH-balanced intimate washes
- Barrier repair: petroleum jelly, ceramide-based creams
- Anti-inflammatory agents: steroids, tacrolimus, pimecrolimus
- Antifungals/antibiotics: based on culture or clinical suspicion
- Aesthetic intervention: laser or PRP for resistant pigment or scars
Clinical Pearls
- Treat the underlying cause first before cosmetic management.
- Always start with least invasive, most biocompatible options in genital skin.
- Educate patients on hygiene, product use, hair removal methods, and clothing.
- Consider psychosexual counseling in patients with body-image concerns.
Summary
| Condition | Diagnosis | Aesthetic Treatment |
| Hyperpigmentation | Clinical + Wood’s lamp | Peels, PRP, lasers |
| Laxity | History + gynecological exam | RF, CO2 laser, PRP |
| Dermatoses | Clinical ± biopsy | Topicals, PRP, scar therapy |
Vulvar Melanosis
1. Introduction
- Definition of Vulvar Melanosis
- Epidemiology and prevalence
- Importance in aesthetic dermatology & sexual medicine
- Clinical relevance: differentiation from malignant lesions
- Patient concern: cosmetic and psychological impact
2. Anatomy and Physiology of the Vulvar Skin
- Vulvar skin histology
- Distribution of melanocytes in the genital area
- Hormonal influence on pigmentation
- Areas most affected (labia minora, majora, perineum)
3. Etiopathogenesis
- Primary (Idiopathic Vulvar Melanosis)
- Secondary (Post-inflammatory hyperpigmentation, chronic irritation, lichen planus, etc.)
- Role of hormones, trauma, and inflammation
- Genetic predisposition
4. Clinical Presentation
- Asymptomatic flat, brown to black macules/patches
- Unilateral or bilateral, irregular but well-defined borders
- Color range: light brown to slate gray
- Sites: labia minora, vestibule, introitus, perineum
Differential Diagnosis
- Vulvar melanoma (most critical to differentiate)
- Lichen planus pigmentosus
- Fixed drug eruption
- Post-inflammatory pigmentation
- Lentigo/simple lentiginosis
- Nevus (junctional or compound)
5. Diagnostic Evaluation
- Clinical Examination: Dermatoscopic evaluation
- Biopsy/Histopathology: Indications for biopsy to rule out melanoma
- Atypical features: asymmetry, rapid growth, variegated color
- Histological features: increased melanin in basal layer without atypia
6. Aesthetic and Medical Management
a. Counseling
- Benign nature of the condition
- Psychological support for aesthetic concerns
- Importance of avoiding unnecessary invasive procedures
b. Topical Treatments
- Hydroquinone 2–4% (limited and cautious use)
- Kojic acid, azelaic acid, arbutin, niacinamide
- Combination depigmenting creams (under supervision)
c. Laser Treatment
- Q-switched Nd:YAG (1064 nm) – Gold standard
- Fractional CO2 laser – cautious and selective use
- Risk of PIH (post-inflammatory hyperpigmentation)
d. Microneedling + Topicals
- Microneedling with depigmenting agents (e.g., tranexamic acid)
7. Complications & Considerations
- PIH due to aggressive treatment
- Skin barrier compromise
- Allergic/irritant reactions from topical agents
- Risk of misdiagnosing melanoma
8. Follow-Up and Monitoring
- Regular photographic documentation
- Repeat dermoscopy in 6–12 months
- Re-biopsy if any sudden change in color, size, or border
9. Academic Case Discussion
- Present real or simulated patient cases:
- History, dermoscopic image, biopsy report, treatment approach
- Ask students to differentiate from melanoma
- Decision-making in choosing aesthetic procedures
10. Key Takeaways for MBBS Aesthetic Students
- Vulvar melanosis is benign but requires expert evaluation
- Dermoscopy and histopathology are key for diagnostic confidence
- Treatment is optional and aesthetic-focused
- Laser and microneedling are advanced approaches
- Importance of multidisciplinary approach – Dermatology, Gynecology, Psychology
📚 Suggested Reading / References
- Bolognia’s Dermatology, Chapter on Pigmentary Disorders
- Fitzpatrick’s Dermatology in General Medicine
- Journal of Clinical and Aesthetic Dermatology (JCAD)
- Vulvar Disorders Guidelines – ACOG, AAD
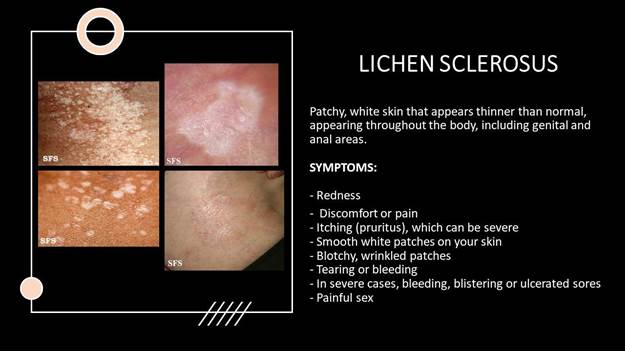
Lichen Sclerosus
1. Introduction
- Definition: Chronic, inflammatory dermatosis predominantly affecting anogenital skin
- Epidemiology: Bimodal distribution – prepubertal girls and postmenopausal women
- Relevance in aesthetic dermatology, gynecology & sexology
- Chronicity, scarring, and quality of life impact
2. Etiology & Pathogenesis
- Etiology: Idiopathic, but multiple contributing factors:
- Autoimmune association (thyroiditis, vitiligo, diabetes)
- Genetic susceptibility
- Hormonal factors (low estrogen)
- Local trauma (Koebner phenomenon)
- Pathogenesis: T-cell mediated chronic inflammation → epithelial atrophy & sclerosis
3. Clinical Features
a. Symptoms
- Itching (intense), burning, soreness
- Dyspareunia (pain during intercourse)
- Dysuria or painful defecation (in severe cases)
b. Signs
- Porcelain-white plaques
- Thinning of skin, wrinkling, fissuring
- Atrophic labia minora, clitoral hood involvement
- Telangiectasia, purpura (due to skin fragility)
- Fusion/scarring leading to anatomical distortion
c. Sites Affected
- Vulva, perineum, perianal region (forming “figure-of-8” or “keyhole” pattern)
- Extragenital LS (rare – trunk, upper limbs)
4. Complications
- Scarring: Labial fusion, clitoral phimosis, introital narrowing
- Functional impairment: Painful intercourse, urinary obstruction
- Malignant transformation: ~5% risk of vulvar squamous cell carcinoma (long-standing cases)
- Psychological distress due to chronicity, sexual dysfunction, and appearance
5. Diagnosis
a. Clinical Diagnosis – Based on history and classical morphology
b. Dermatoscopic Features:
- White structureless areas
- Telangiectasia, follicular plugging
c. Histopathology (when needed):
- Epidermal atrophy
- Basal cell degeneration
- Homogenized collagen in upper dermis
- Band-like lymphocytic infiltrate
d. Indications for Biopsy:
- Atypical lesions
- Suspicion of malignancy
- Poor response to therapy
6. Management Approach
a. Patient Counseling
- Chronic, relapsing course
- Importance of adherence to treatment
- Monitoring for complications
b. Medical Treatment
- Topical High-potency Corticosteroids:
- Clobetasol propionate 0.05% ointment (first-line)
- Application protocol: Daily × 4 weeks → taper
- Topical Calcineurin Inhibitors:
- Tacrolimus/pimecrolimus for maintenance (off-label)
- Other Options:
- Topical estrogen (in postmenopausal)
- Oral retinoids (in resistant cases)
- Phototherapy (narrowband UVB)
7. Aesthetic & Functional Interventions
a. PRP (Platelet-Rich Plasma):
- Emerging therapy for vulvar rejuvenation
- Promotes tissue regeneration & reduces symptoms
b. Laser Therapy (Selective Use):
- Fractional CO₂ laser
- Improves vulvar texture, flexibility, dyspareunia
c. Surgical Management (Advanced Cases):
- Lysis of adhesions
- Introital widening
- Vulvectomy (for malignant transformation)
8. Follow-Up and Monitoring
- Regular follow-up every 3–6 months
- Monitor for malignant transformation signs (new nodules, bleeding, non-healing ulcers)
- Long-term use of maintenance therapy to prevent flares
9. Differential Diagnoses
- Lichen planus
- Vulvar intraepithelial neoplasia (VIN)
- Chronic candidiasis
- Vulvar atrophy (senile)
- Vitiligo (non-inflammatory depigmentation)
10. Academic Case Discussion
- Case 1: A postmenopausal woman with chronic itching and white vulvar plaques
- Case 2: Prepubertal girl with anal-vulvar itching and scarring
- Evaluate based on history, examination, biopsy, and develop treatment plan
- Emphasis on counseling, aesthetics, and long-term follow-up
11. Key Points for MBBS Aesthetic Academic Students
- LS is chronic, inflammatory and can lead to anatomical, functional, and psychological consequences
- Early diagnosis and corticosteroid therapy prevent scarring and cancer
- Aesthetic interventions (PRP, laser) can improve patient comfort and cosmetic outcomes
- Multidisciplinary care: Dermatology, Gynecology, Psychology, Aesthetic Medicine
📚 Recommended References
- Fitzpatrick’s Dermatology in General Medicine
- Bolognia: Dermatology – Vulvar Disorders
- ACOG Guidelines on Vulvar Skin Disorders
- British Association of Dermatologists Patient Information Leaflet
- Journal of the European Academy of Dermatology and Venereology (JEADV)
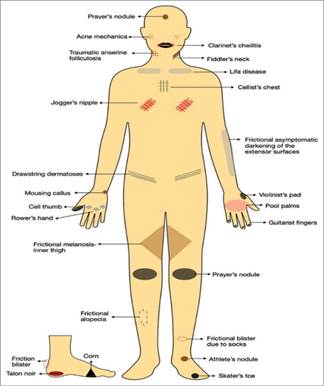
Frictional Pigmentation
1. Introduction
- Definition: Chronic localized hyperpigmentation caused by repeated friction, pressure, or irritation on the skin
- Importance: Common in South Asian and darker skin types
- Relevance in aesthetic dermatology, particularly in skin of color patients
- Aesthetic concern due to disfigurement, especially in exposed or intimate areas
2. Etiopathogenesis
- Repeated friction → epidermal hyperplasia → increased melanogenesis
- Mechanical triggers:
- Tight clothing (waistbands, undergarments, brassieres)
- Rubbing from belts, sandals, hijab/veil edges
- Intertriginous friction: thighs, axilla, groin, neck folds
- Cosmetic practices: loofahs, scrubbing
- Role of sweat, obesity, poor hygiene, heat
- Melanocyte stimulation by low-grade trauma → persistent post-inflammatory hyperpigmentation (PIH)
3. Common Clinical Sites
- Nape of the neck
- Inner thighs
- Axillae
- Groin/genital folds
- Abdomen (waistband area)
- Ankles (from footwear straps)
- Underarms, inframammary area (in females)
4. Clinical Features
- Hyperpigmented, ill-defined, symmetric or asymmetric patches
- Brown to grayish-black coloration
- No scaling, no induration
- Usually asymptomatic (may be mildly itchy if irritation persists)
5. Differential Diagnosis
| Condition | Key Differentiators |
| Acanthosis Nigricans | Velvety texture, insulin resistance association |
| Post-inflammatory hyperpigmentation | Follows eczema, infection, or trauma |
| Lichen planus pigmentosus | Ashy-gray, inflammatory history, lichen planus elsewhere |
| Dermatosis Papulosa Nigra (DPN) | Papular lesions |
| Lichen simplex chronicus | Thickened skin due to chronic scratching |
| Fixed drug eruption | Recurrent at same site, dusky patches post-drug exposure |
6. Diagnostic Evaluation
- Clinical diagnosis (primarily visual inspection)
- Dermoscopy: May show pigment network, accentuated skin markings
- Wood’s lamp: To assess epidermal vs dermal pigmentation
- Skin biopsy: Rarely needed; shows basal layer hyperpigmentation and epidermal thickening
7. Management Approach
a. Elimination of Cause
- Patient education: avoid tight clothing, change friction-causing habits
- Use soft fabrics, breathable undergarments
- Reduce friction in obese patients: weight loss counseling, anti-chafing powders
b. Topical Therapy
- Depigmenting agents:
- Hydroquinone 2–4% (short-term use)
- Kojic acid, azelaic acid, niacinamide
- Alpha arbutin, licorice extract
- Keratolytic agents:
- Lactic acid, glycolic acid (6–12%)
- Urea-based creams
- Topical retinoids:
- Tretinoin 0.025–0.05% (for thickened skin + pigmentation)
c. Adjunctive Treatments
- Sunscreen application – especially on exposed areas (e.g., neck)
- Barrier creams or moisturizers – reduce friction and repair skin barrier
8. Aesthetic Treatment Options
a. Chemical Peels
- Superficial peels (Mandelic, Lactic, Glycolic acid)
- Weekly or bi-weekly sessions over 6–8 weeks
- Caution in skin of color – avoid strong peels to reduce PIH risk
b. Laser Treatments
- Q-switched Nd:YAG 1064 nm – for dermal pigmentation
- Low-fluence sessions at intervals
- Risk: PIH if aggressive in darker skin types
c. Microneedling + Topical Depigmenting Agents
- Enhances penetration of actives like tranexamic acid or vitamin C
- Safer option for intimate or sensitive areas
9. Complications
- Psychological impact due to cosmetic disfigurement
- Long-standing pigmentation may be difficult to reverse
- Risk of treatment-induced PIH, especially with aggressive modalities
10. Follow-Up & Prognosis
- Reversible if friction is removed early
- Pigmentation fades over months with combined therapy
- Maintenance needed in recurrent friction-prone areas
- Periodic reassessment of cosmetic progress and patient satisfaction
11. Case Discussion & Clinical Scenarios
- Case 1: Obese female with inner thigh pigmentation from friction + tight leggings
- Case 2: Male patient with pigmentation over neck due to collar friction
- Case 3: Adolescent girl with dark underarms due to shaving and tight clothing
- Discuss diagnosis, treatment plan, and aesthetic counseling
12. Key Learning Points for MBBS Aesthetic Students
- Frictional pigmentation is common, benign, and preventable
- History and inspection are key to diagnosis
- Topical and aesthetic treatments must be selected carefully in darker skin types
- Counseling on habits and lifestyle is essential
- Multimodal therapy (peels, topicals, microneedling) yields best results
Advance Diploma Course in Aesthetic Dermatology & Sexology
- Day 02
- Clinical Sexology – Sexual Dysfunction & Male & Female Sexual Dysfunctions – ED, PE, Low Libido, Vaginal Dryness
- Hormone Balancing, PRP
- O-Shot, P-Shot
- Role of Cosmeceuticals & Nutra-pharma in Sexual Wellness
![]() Clinical Sexology
Clinical Sexology
Module 1: Sexual Health – Anatomy & Physiology
- Male and female sexual anatomy (penis, clitoris, vagina, erectile tissue, pelvic floor)
- Neurovascular and hormonal regulation
- Hormones involved: Testosterone, Estrogen, Oxytocin, Dopamine
- Human sexual response cycle (Desire → Arousal → Orgasm → Resolution)
Module 2: Classification & Diagnosis of Sexual Dysfunction
- WHO / DSM-5 / ICD-11 criteria
- Types of dysfunction:
- Male: ED, PE, Hypoactive Sexual Desire
- Female: FSIAD, Vaginal Atrophy, Anorgasmia
- Biopsychosocial model of dysfunction
- Sexual history taking (PLISSIT model)
- Patient questionnaires: IIEF, FSFI
Men Erectile Dysfunction (ED)
Course Structure:
| Module | Topic |
| 1 | Introduction & Physiology of Penile Erection |
| 2 | Epidemiology & Classification of Erectile Dysfunction |
| 3 | Etiology: Organic, Psychological & Mixed |
| 4 | History Taking & Clinical Evaluation |
| 5 | Investigations & Diagnostic Tools |
| 6 | Pharmacological Management |
| 7 | Lifestyle & Psychosexual Therapy |
| 8 | Aesthetic & Regenerative Interventions |
Module-wise Breakdown:
Module 1: Introduction & Physiology of Penile Erection
- Anatomy of penis: Corpora cavernosa, corpus spongiosum, vascular supply
- Neurovascular regulation of erection
- Role of NO (Nitric Oxide) and cGMP pathway
- Endocrinology: Role of testosterone and other hormones
- Types of erection: Reflexogenic, Psychogenic, Nocturnal
Module 2: Epidemiology & Classification
- Global and regional prevalence (including South Asia)
- Classification:
- Organic (vascular, neurogenic, hormonal, drug-induced)
- Psychogenic (anxiety, relationship issues, trauma)
- Mixed ED
- Associated comorbidities: Diabetes, CVD, obesity, smoking
Module 3: Causes of Erectile Dysfunction
- Vascular: Atherosclerosis, endothelial dysfunction
- Neurological: Spinal cord injuries, multiple sclerosis
- Endocrine: Hypogonadism, thyroid dysfunction, hyperprolactinemia
- Drug-induced: Antihypertensives, antidepressants, alcohol, smoking
- Psychological: Performance anxiety, depression
- Post-surgical or trauma-related
Module 4: History Taking & Clinical Evaluation
- Sensitive patient communication techniques
- Sexual health history (IIEF – International Index of Erectile Function)
- Physical examination: Secondary sexual characteristics, penile/scrotal exam
- Mental health assessment
- Screening for cardiovascular risk
Module 5: Investigations & Diagnostic Tools
- Blood tests: Testosterone, LH, FSH, Prolactin, TSH, HbA1c, Lipid profile
- Penile Doppler ultrasound with injection test
- Nocturnal Penile Tumescence (NPT) test
- Psychological evaluation if needed
- Penile biothesiometry (optional)
Module 6: Pharmacological Treatment
- PDE-5 Inhibitors: Sildenafil, Tadalafil, Vardenafil
- Mechanism of action
- Dosing guidelines
- Contraindications (e.g., nitrate use)
- Side effects
- Intracavernosal Injections: Alprostadil
- Vacuum Erection Devices (VED)
- Hormone Replacement Therapy (TRT) for hypogonadism
- Indications and risks
- Monitoring protocols
Module 7: Lifestyle & Psychosexual Counseling
- Lifestyle modifications:
- Diet, weight loss, smoking cessation
- Regular aerobic exercise
- Stress reduction: Meditation, yoga, counseling
- Psychosexual therapy and couple’s therapy
- Addressing unrealistic expectations
- Referral to psychiatrist/sex therapist if needed
Module 8: Aesthetic & Regenerative Interventions
8.1 Platelet-Rich Plasma (PRP) – “P-Shot”
- Mechanism: Angiogenesis, nerve regeneration
- Indications and outcomes
- Procedure steps, safety, and aftercare
8.2 Low-Intensity Shockwave Therapy (LI-ESWT)
- Mechanism: Neovascularization, smooth muscle repair
- Evidence-based outcomes
- Protocol and machine settings
8.3 Stem Cell Therapy & Exosomes (Advanced/Research-level)
- Emerging therapies
- Ethical and legal considerations
8.4 Aesthetic Counselling
- Addressing body image, genital self-perception
- Penile enhancement myths vs reality
Female Sexual Dysfunction (ED)
Course Objectives:
By the end of the course, MBBS students will be able to:
- Understand the anatomy and physiology of female sexual response
- Classify and diagnose different types of female sexual dysfunctions
- Take detailed sexual and psychosocial histories with sensitivity
- Conduct relevant investigations for hormonal or structural issues
- Explore conventional, hormonal, psychological, and aesthetic treatments
- Incorporate PRP, laser, fillers, and other regenerative techniques into management
Course Structure:
| Module | Topic |
| 1 | Female Sexual Anatomy & Physiology |
| 2 | Sexual Response Cycle & Hormonal Regulation |
| 3 | Classification of Female Sexual Dysfunctions |
| 4 | History Taking, Assessment & Diagnosis |
| 5 | Psychosexual Aspects & Counseling |
| 6 | Pharmacological & Hormonal Treatments |
| 7 | Aesthetic & Regenerative Treatments |
Module 1: Female Sexual Anatomy & Physiology
- Anatomy: Clitoris, G-spot, A-spot, vagina, vulva, labia, Skene & Bartholin glands
- Nerve supply (pudendal, pelvic) and blood supply
- Pelvic floor musculature and its role in orgasm and arousal
- Physiology of arousal, lubrication, engorgement, and orgasm
Module 2: Sexual Response Cycle & Hormonal Regulation
- Phases: Desire → Arousal → Plateau → Orgasm → Resolution
- Role of hormones:
- Estrogen: vaginal health, lubrication
- Testosterone: libido and sexual drive
- Oxytocin & dopamine: bonding and pleasure
- Menopause and its impact on sexual function
Module 3: Classification of Female Sexual Dysfunctions
As per DSM-5 and ICD-11:
- Female Sexual Interest/Arousal Disorder (FSIAD)
- Female Orgasmic Disorder
- Genitopelvic Pain/Penetration Disorder (GPPPD)
- Vaginismus
- Vulvodynia and dyspareunia
- Hypoactive Sexual Desire Disorder (HSDD)
Module 4: History Taking, Assessment & Diagnosis
- Sexual history using PLISSIT and BETTER models
- Psychosocial factors: relationship status, trauma history, stress
- Physical examination: vaginal atrophy, dryness, tone
- Use of validated tools:
- FSFI (Female Sexual Function Index)
- GRISS (Golombok-Rust Inventory of Sexual Satisfaction)
- Hormonal testing: Estradiol, Testosterone, FSH, LH, SHBG, TSH
- Vaginal pH, elasticity assessment
Module 5: Psychosexual Aspects & Counseling
- Psychosocial contributors: fear, trauma, self-image, relationship issues
- Communication training: empathetic, non-judgmental consultations
- Role of cognitive-behavioral therapy (CBT)
- Couples therapy basics
- Referral pathways: Psychologist, sex therapist, gynecologist
Module 6: Pharmacological & Hormonal Management
A. Desire Disorders
- Flibanserin (FDA-approved for HSDD)
- Bremelanotide (injectable on-demand drug for HSDD)
- Off-label testosterone therapy (gel/cream)
- Herbal supplements: maca root, ginseng, tribulus terrestris
B. Arousal & Orgasm Disorders
- Sildenafil (experimental use)
- Pelvic floor therapy, vibrator therapy
- Lubricants & vaginal moisturizers
C. Vaginal Dryness & Dyspareunia
- Topical estrogen cream or rings
- DHEA vaginal suppositories
- Hyaluronic acid gel
Module 7: Aesthetic & Regenerative Treatments
A. Platelet-Rich Plasma (PRP) – O-Shot®
- Mechanism: regeneration of nerves, increase in lubrication and sensitivity
- Procedure protocol and aftercare
- Indications: Low libido, orgasmic dysfunction, vaginal dryness
B. Laser Vaginal Rejuvenation (CO₂/Er:YAG Laser)
- Indications: Vaginal atrophy, laxity, dryness, dyspareunia
- Mechanism: Collagen remodeling, improved elasticity
- Procedure steps and safety considerations
C. Vaginal Fillers
- Hyaluronic acid-based fillers for hydration and tone
- G-spot & A-spot enhancement techniques
- Precautions and side effects
D. Botulinum Toxin for Vaginismus
- Use of Botox in pelvic floor hypertonicity
- Indications and dosing
E. Radiofrequency & Ultrasound Therapy
- For vaginal tightening and urinary incontinence
- Combined benefits for sexual function
Module 8: Case-Based Discussions & Clinical Integration
- Case 1: Perimenopausal woman with dryness and low libido
- Case 2: Young woman with vaginismus and marital stress
- Case 3: Orgasmic dysfunction with antidepressant use
- Role-play on sensitive counseling and patient consent
- Discussion on ethical practice, informed consent, and privacy
Low Libido in Females
- Understand the biological, psychological, and social determinants of sexual desire in women
- Diagnose Hypoactive Sexual Desire Disorder (HSDD) and distinguish it from other dysfunctions
- Evaluate hormonal, physiological, and relational contributors
- Apply pharmacological, psychosexual, and aesthetic treatment strategies
- Communicate effectively and ethically about female sexual health
- Incorporate regenerative & aesthetic medicine tools like PRP, hormonal creams, and laser therapy
Course Outline:
| Module | Topic |
| 1 | Female Sexual Desire – Anatomy & Physiology |
| 2 | Epidemiology & Classification of Low Libido |
| 3 | Causes of Low Libido: Multifactorial Model |
| 4 | Clinical Assessment & Diagnostic Tools |
| 5 | Psychological & Relationship Factors |
| 6 | Medical & Hormonal Management |
| 7 | Aesthetic & Regenerative Interventions |
Module-wise Detailed Content:
Module 1: Female Sexual Desire – Anatomy & Physiology
- Central and peripheral regulation of libido
- Role of brain regions: limbic system, hypothalamus
- Neurochemical pathways: dopamine, serotonin, oxytocin
- Endocrine factors: estrogen, progesterone, testosterone, DHEA
- Role of clitoris, vaginal innervation, and genital sensory input
Module 2: Epidemiology & Classification
- Prevalence of Hypoactive Sexual Desire Disorder (HSDD)
- DSM-5 vs ICD-11 classification
- Types:
- Acquired vs lifelong
- Generalized vs situational
- Impact on quality of life and relationships
- Cultural and regional perspectives, including South Asia
Module 3: Causes of Low Libido
A. Biological Factors
- Hormonal imbalance (low estrogen/testosterone)
- Menopause and perimenopause
- Thyroid dysfunction, chronic illness, anemia
- Medications: SSRIs, contraceptives, antihypertensives
B. Psychological Factors
- Depression, anxiety
- Past trauma or sexual abuse
- Negative body image, low self-esteem
C. Relational & Social Factors
- Partner issues
- Lack of emotional connection
- Cultural shame or stigma
- Parenting and fatigue
Module 4: Clinical Assessment & Diagnosis
- Taking a detailed and sensitive sexual history
- Use of validated tools:
- FSFI (Female Sexual Function Index)
- Decreased Sexual Desire Screener (DSDS)
- Hormonal tests: Testosterone, estradiol, SHBG, DHEA, TSH
- Rule out other sexual dysfunctions: arousal, orgasm, pain
- General and pelvic examination
- Mental health and relationship screening
Module 5: Psychological & Relationship Counseling
- Basic sex therapy and CBT approaches
- PLISSIT model (Permission, Limited Information, Specific Suggestions, Intensive Therapy)
- Addressing myths, guilt, and communication barriers
- Couple therapy
- Stress management techniques
Module 6: Medical & Hormonal Management
A. Pharmacological
- Flibanserin (Addyi): serotonin receptor modulator
- Indicated in premenopausal HSDD
- Side effects, contraindications
- Bremelanotide (Vyleesi): melanocortin receptor agonist
- On-demand injectable treatment for HSDD
B. Hormonal Therapy
- Testosterone therapy (transdermal gel or cream)
- Off-label use in postmenopausal women
- Monitoring protocol
- Estrogen therapy (local vaginal rings or creams)
- DHEA intravaginal suppositories
Module 7: Aesthetic & Regenerative Medicine Options
A. PRP (O-Shot®) – Platelet-Rich Plasma
- Increases sensitivity and arousal
- Protocol, safety, consent, and outcomes
- Indicated in libido loss, orgasmic dysfunction
B. Laser Vaginal Rejuvenation
- CO₂ or Er:YAG laser
- Enhances lubrication, improves elasticity, improves blood flow
- Indirect benefit on desire and comfort
C. Radiofrequency & Ultrasound Therapy
- Improves pelvic floor tone and sexual satisfaction
D. Botox (in special cases)
- For vaginismus contributing to secondary low desire
E. Aesthetic Counseling
- Genital appearance and body image impact on desire
- Vulvar skin treatments, pigmentation reduction
✅ Module 8: Case-Based Learning, Communication & Ethics
- Case 1: Young woman on SSRI with HSDD
- Case 2: Postmenopausal woman with low libido and vaginal dryness
- Case 3: Couple in therapy with mismatched desire levels
- Teaching students empathetic communication and cultural sensitivity
- Legal and ethical considerations in aesthetic sexology practice
- Informed consent and confidentiality protocol
Vaginal Dryness
Course Objectives:
Upon completion, students will be able to:
- Understand the anatomy and physiology of vaginal lubrication
- Identify causes of vaginal dryness across different life stages
- Diagnose Genitourinary Syndrome of Menopause (GSM) and related conditions
- Implement both hormonal and non-hormonal medical treatments
- Apply regenerative and aesthetic techniques (e.g., laser, PRP, RF)
- Communicate with patients ethically and sensitively
Course Modules:
| Module No. | Topic |
| 1 | Anatomy & Physiology of Vaginal Lubrication |
| 2 | Causes & Classification of Vaginal Dryness |
| 3 | History Taking & Diagnostic Evaluation |
| 4 | Hormonal & Medical Management |
| 5 | Non-Hormonal and Lifestyle Approaches |
| 6 | Aesthetic & Regenerative Interventions |
| 7 | Psychosexual Impact & Communication |
| 8 | Case Studies and OSCE Practice |
Module-Wise Details:
Module 1: Anatomy & Physiology
- Vaginal wall structure and secretory glands (Bartholin, Skene)
- Estrogen’s role in maintaining vaginal moisture and elasticity
- Neurovascular supply and sensory innervation
- Role of vaginal microbiome and pH balance
Module 2: Causes & Classification
- Life-stage Related:
- Menopause, perimenopause (GSM)
- Postpartum, lactation
- Medical/Pharmacological:
- SSRIs, antihistamines, chemotherapy
- Low-estrogen contraceptives
- Pathological:
- Sjögren’s syndrome, lichen sclerosus
- Atrophic vaginitis
- Lifestyle/Psychogenic:
- Smoking, dehydration, stress
- Past trauma and relationship issues
Module 3: Clinical Assessment
- Comprehensive sexual and gynecologic history
- Use of tools: FSFI (Female Sexual Function Index), GSM Questionnaire
- Vaginal pH, elasticity, and moisture evaluation
- Pelvic exam & inspection
- Hormone testing: Estradiol, FSH, DHEA, SHBG
- Differential diagnosis with infections, dermatological conditions
Module 4: Hormonal & Pharmacologic Treatment
- Local Estrogen Therapy:
- Creams, rings, vaginal tablets (estradiol, estriol)
- Dosing guidelines, follow-up care
- Contraindications: hormone-sensitive cancers
- Systemic Hormone Therapy (HRT):
- When combined with hot flashes or GSM
- Risk-benefit assessment
- Other Hormonal Agents:
- DHEA suppositories (FDA-approved)
- Testosterone therapy (off-label for libido)
Module 5: Non-Hormonal & Lifestyle Interventions
- Vaginal moisturizers vs lubricants (water/silicone/oil-based)
- Hyaluronic acid vaginal gels
- Aloe vera, sea buckthorn, plant estrogens
- Intimacy exercises and sexual wellness routines
- Hydration, smoking cessation, regular sexual activity
Module 6: Aesthetic & Regenerative Interventions
A. Laser Vaginal Rejuvenation (CO₂ or Er:YAG)
- Enhances collagen and mucosal regeneration
- Effective for GSM and vaginal dryness
- Procedure steps, patient selection, outcomes
B. PRP (Platelet-Rich Plasma – O-Shot®)
- Enhances nerve sensitivity and vascularity
- Step-by-step injection technique
- Results and patient education
C. Radiofrequency (RF) & Ultrasound
- Non-invasive, improves tissue hydration and elasticity
D. Hyaluronic Acid Fillers (experimental use)
- Improves hydration and volume in severe atrophic cases
Module 7: Psychosexual Impact & Counseling
- Impact of dryness on intimacy and self-esteem
- Counseling techniques: PLISSIT model
- Culturally sensitive communication
- Partner involvement and education
- Ethical principles: confidentiality, consent, non-judgment
- Hormone Balancing, PRP
- O-Shot, P-Shot
Course Objectives:
By the end of the course, students will be able to:
- Understand hormonal regulation in male and female sexual function
- Diagnose and manage hormone imbalances clinically and ethically
- Describe the principles and mechanisms of PRP therapy
- Perform or observe the P-Shot® procedure for male sexual enhancement
- Evaluate patients for suitability and consent for regenerative sexual therapies
- Integrate hormonal and PRP-based approaches for ED, low libido, and penile rejuvenation
Course Structure:
| Module | Topic |
| 1 | Introduction to Hormone Balancing |
| 2 | Male & Female Hormonal Pathways in Sexual Health |
| 3 | Clinical Assessment & Diagnostic Workup |
| 4 | Hormone Replacement Therapy (HRT) – Male & Female |
| 5 | Introduction to PRP in Aesthetic & Sexual Medicine |
| 6 | P-Shot®: Indications, Procedure, Outcomes |
| 7 | Ethics, Consent & Medicolegal Considerations |
| 8 | Case Studies, OSCE & Clinical Simulation |
Module-Wise Details:
Module 1: Introduction to Hormone Balancing
- Role of hormones in sexual function, libido, energy, and aging
- Concept of “Hormone Optimization” in aesthetic practice
- Differences between conventional HRT and bioidentical hormone therapy
- Hormone decline with age – “andropause” and “menopause”
Module 2: Sexual Hormonal Pathways
A. In Males
- Hypothalamic-Pituitary-Gonadal (HPG) Axis
- Testosterone (free & total), DHT, LH, FSH, SHBG
- Cortisol and thyroid interplay
- Impact on libido, erection, energy
B. In Females
- Estrogen, Progesterone, Testosterone
- DHEA, cortisol, thyroid profile
- Role in vaginal health, libido, mood
Module 3: Clinical Assessment & Workup
- Full sexual and fatigue history
- Hormone panel interpretation
- FSFI, IIEF scores (for sexual function)
- Saliva, serum, and urine hormone testing
- Nutritional and lifestyle assessment
Module 4: Hormone Replacement Therapy (HRT)
For Males:
- Testosterone therapy: gels, injections, pellets
- Monitoring PSA, hematocrit, estradiol
- Risks: fertility suppression, polycythemia, gynecomastia
For Females:
- Estrogen (oral, transdermal, vaginal), Progesterone
- DHEA, testosterone cream (compounded, off-label use)
- Managing GSM, libido loss, mood changes
Module 5: Introduction to PRP in Sexual & Aesthetic Medicine
- PRP composition: platelets, growth factors, cytokines
- Biological effects: angiogenesis, nerve regeneration, collagen stimulation
- PRP preparation protocol: double-spin method
- Safety and efficacy, autologous nature
Module 6: P-Shot® (Priapus Shot) – Male Sexual Enhancement
- Indications:
- Erectile Dysfunction (mild to moderate)
- Penile girth enhancement
- Peyronie’s disease
- Sexual confidence/psychogenic ED
- Contraindications:
- Active infection, bleeding disorders, unrealistic expectations
- Procedure Steps:
- Consent and photography (if applicable)
- Numbing cream and penile block
- PRP extraction and activation
- Intracavernosal injection technique (2–4 quadrants)
- Post-care, vacuum device use, follow-up protocols
- Expected Outcomes & Timelines
- Clinical safety and complications (pain, swelling, rare fibrosis)
Module 7: Medicolegal & Ethical Considerations
- Informed consent documentation
- Off-label hormone use and PRP disclaimers
- Transparency in results and expectations
- Contraindications and ethics in sexual enhancement therapy
Cosmeceuticals & Nutra-pharma in Sexual Wellness
Course Objectives:
By the end of the course, students will be able to:
- Understand how nutraceuticals, herbal supplements, and cosmeceuticals influence sexual function
- Identify commonly used agents that enhance libido, erectile function, lubrication, and mood
- Understand the clinical evidence behind topical and ingestible formulations
- Advise patients ethically on complementary wellness strategies for sexual dysfunction
- Integrate nutra-pharma into aesthetic and sexual medicine practice safely and responsibly
Course Modules:
| Module No. | Topic |
| 1 | Introduction to Sexual Wellness & Functional Aesthetics |
| 2 | Basics of Cosmeceuticals and Nutra-Pharma |
| 3 | Nutra-Pharma in Male Sexual Health |
| 4 | Nutra-Pharma in Female Sexual Health |
| 5 | Cosmeceutical Agents in Genital Aesthetics |
| 6 | Clinical Evidence & Safety |
| 7 | Counseling, Ethics & Regulation |
| 8 | OSCE + Case-Based Learning |
Module-Wise Breakdown:
Module 1: Introduction to Sexual Wellness
- Understanding “Sexual Wellness” as part of holistic aesthetic care
- Psychosomatic and hormonal aspects
- Integration with aesthetic gynecology/urology and lifestyle medicine
Module 2: Cosmeceuticals & Nutra-Pharma Basics
- Definitions and classifications:
- Cosmeceuticals: Topical agents with pharmacological benefit
- Nutra-pharma/Nutraceuticals: Oral supplements with therapeutic roles
- Mechanisms:
- Boosting nitric oxide, testosterone, estrogen balance
- Modulating stress, mood, inflammation, circulation
Module 3: Nutra-Pharma in Male Sexual Wellness
- L-Arginine & L-Citrulline – Vasodilation via nitric oxide
- Zinc, Vitamin D, Selenium – Testosterone regulation
- DHEA – Hormonal precursor
- Ashwagandha, Maca Root, Tongkat Ali – Adaptogens for libido and energy
- Tribulus terrestris, Fenugreek – Testosterone-boosting herbs
- Ginkgo biloba – Circulatory support for erectile health
- Omega-3 & Antioxidants – Sperm quality, penile endothelial function
Module 4: Nutra-Pharma in Female Sexual Wellness
- Isoflavones & Phytoestrogens – Estrogen support in peri/post-menopause
- Vitamin E, Omega-3, B-complex – Vaginal health & lubrication
- Maca, Damiana, Ginseng – Libido enhancement
- Evening Primrose Oil – Vaginal tissue hydration
- Magnesium, Adaptogens – Mood, stress & fatigue relief
- Role in managing Female Sexual Interest/Arousal Disorder (FSIAD)
Module 5: Cosmeceuticals in Genital Aesthetics
- Topical Hyaluronic Acid – For vulvar and vaginal hydration
- Niacinamide, Aloe Vera – Brightening, soothing vulvar pigmentation
- Lactic Acid & Prebiotic Washes – Maintaining healthy vaginal flora
- Natural lubricants vs synthetic agents – Cosmetic & sexual use
- Vaginal rejuvenation serums – Marketed ingredients and ethics
- Evaluation of safety, pH, and allergenicity
Module 6: Evidence-Based Use & Clinical Studies
- Review of key RCTs and meta-analyses
- Clinical use guidelines (ISSM, AACE, etc.)
- Evidence grade for each major supplement and compound
- Limitations and placebo effects in sexual wellness trials
Module 7: Ethics, Patient Education & Regulation
- OTC vs prescription-based supplements
- Avoiding exaggerated claims (anti-aging, aphrodisiac)
- Adverse effects, herb-drug interactions
- Cultural sensitivity and sexual health communication
- Regulatory bodies: DGDA (BD), FDA (US), EMA (EU)
Module 8: OSCE & Case-Based Discussion
- Case 1: Young male with stress-related ED asking about Ashwagandha
- Case 2: Menopausal woman with vaginal dryness & libido loss interested in Maca and topical estrogen-free options
- Case 3: Male patient already on PDE5 inhibitors exploring PRP + L-arginine
- Practice:
- Supplement counseling OSCE
- Product label analysis
Evidence appraisal activity
Leave a Reply